REVIEW ARTICLE
TRANSLATION, RELIABILITY, AND VALIDITY OF THE TRUNK IMPAIRMENT SCALE IN A POLISH POPULATION AFTER STROKE
Joanna MAŁECKA, PT, PhD1, Magdalena GOLIWĄS, PT, PhD2, Katarzyna ADAMCZEWSKA, PT, PhD1, Jacek LEWANDOWSKI Full professor, PT PhD2, Geert VERHEYDEN Prof, PT, PhD, FESO3,4 and Dawid ŁOCHYŃSKI, Assoc Prof, PT, PhD1
From the 1Department of Neuromuscular Physiotherapy, Poznan University of Physical Education, Poznan, 2Department of Musculoskeletal Rehabilitation, Poznan University of Physical Education, Poznan, Poland, 3Department of Rehabilitation Sciences, KU Leuven – University of Leuven, Leuven, and 4Leuven Brain Institute, KU Leuven – University of Leuven, Leuven, Belgium
Objective: This study was conducted to estimate the reliability and validity of the translated and culturally adapted Polish version of the Trunk Impairment Scale in post-stroke patients and to determine the strength of the relationship between trunk and upper limb physical function after stroke.
Design: The Polish version of the Trunk Impairment Scale was developed through cultural adaptation. Internal consistency, test–retest reliability, and inter-rater reliability were determined, and construct validity was evaluated by analysing the Polish version of the Trunk Impairment Scale, the Polish version of the Fugl-Meyer Assessment Scale, and the Polish version of the Action Research Arm Test.
Participants: Eighty patients with diagnosed stroke in the subacute and chronic stages.
Results: The internal consistency for the Polish version of the Trunk Impairment Scale was excellent (α = 0.85–0.91). Test–retest and inter-rater reliability were almost perfect (ICC = 0.94–1.0, κ = 0.92–1.0). Construct validity was moderate (rho = 0.71–0.76). A moderate correlation was also found between the Polish version of the Trunk Impairment Scale and Polish version of the Action Research Arm Test total scores (rho = 0.60).
Conclusion: The Polish version of the Trunk Impairment Scale is a reliable and moderately valid outcome measure to assess trunk impairment in Polish stroke survivors. Trunk function is moderately related to gross and fine motor skills of the arm, hand, and fingers among individuals with stroke.
LAY ABSTRACT
Two primary objectives were pursued in this study. The first aim was to evaluate the diagnostic utility of the newly developed Polish version of the Trunk Impairment Scale. The second was to examine the relationship between trunk and upper extremity function. A total of 80 post-stroke participants were enrolled. The Trunk Impairment Scale was translated into Polish, and subsequently, the reliability and validity of the Polish version of the Trunk Impairment Scale were calculated. Furthermore, the correlation between the Polish version of the Trunk Impairment Scale and the Polish version of the Action Research Arm Test was analysed. The results showed that the Polish version of the Trunk Impairment Scale is a highly reliable and moderately valid outcome measure for assessing individuals in the Polish population after stroke. Moreover, a moderate relationship between trunk function and upper extremity activity was demonstrated.
Key words: stroke; outcome measure; TIS; FMA; ARAT; trunk impairment.
Citation: J Rehabil Med 2026; 58: jrm44789. DOI: https://doi.org/10.2340/jrm.v58.44789.
Copyright: © 2026 The Author(s). Published by MJS Publishing, on behalf of the Foundation for Rehabilitation Information. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/).
Submitted: Sept 12, 2025; Accepted after revision: Jan 22, 2026; Published: Mar 10, 2026.
Correspondence address: Joanna Małecka, Department of Neuromuscular Physiotherapy, Poznan University of Physical Education, Poznan, Poland. E-mail: malecka@awf.poznan.pl
Trunk control is the main indicator of functional recovery after stroke (1, 2).There is a link between trunk performance, balance, gait, and functional outcome in stroke patients (3, 4). Physical rehabilitation of trunk function is essential; thus, reliable and valid outcome measures are critical for assessing the level of trunk function impairment in clinical practice.
The trunk plays an integral role in postural stability by supporting controlled movement of the extremities during motor tasks (5, 6). The enhancement of trunk stability and control is regarded as a fundamental requirement for upper extremity function and effective hand use (7). Trunk stability affects shoulder stability, thereby enhancing elbow, wrist, and finger motion. A stable trunk establishes a firm base for the force produced by the extremities (8). It has previously been reported that trunk physical function is linked to upper extremity functional performance after stroke (4, 9, 10, 11). Thus, it is important to assess upper extremity function in addition to trunk performance.
The Trunk Impairment Scale (TIS) was designed to assess motor impairment of the trunk after stroke (12). The TIS has been translated into several languages in previous studies (1, 13, 15–20), and this outcome measure has demonstrated good psychometric properties (1, 14–19). The TIS has demonstrated low to excellent internal consistency in patients after stroke (α = 0.61–0.97) (1, 14, 15, 18, 20). The test–retest reliability, calculated using intraclass correlation coefficient values, is moderate to excellent (r = 0.73–0.97) (1, 5, 6, 9). The inter-rater reliability values for the total and subscale scores range from 0.63 to 0.99 in post-stroke patients (1, 14, 15, 18). Studies examining the validity have demonstrated moderate, good, or high (19, 20) correlations (rho = 0.56–0.86) between the TIS and the total scores of other outcome measures, such as the Trunk Control Test, Barthel Index, Berg Balance Scale, Fugl Meyer Assessment Balance, and Rivermead Mobility Index (12, 18, 19).
There is no culturally adapted and validated Polish tool specifically designed to assess trunk physical function that could establish the construct validity of the TIS. Furthermore, the relationship between the control of selective trunk movements and the fine control (e.g., pinching, grasping) of the upper extremities has never been studied using dedicated measurement tools such as the TIS and ARAT (21). Both outcome measures are considered adequate for assessing postural control of the trunk (12) and dexterity of upper-extremity movements after stroke (22). Thus, assessing these factors may provide a new perspective on therapeutic strategies to improve trunk control and upper limb function after stroke. The present study was conducted to estimate the reliability and validity of the translated and culturally adapted Polish version of the TIS in a population of post-stroke patients. The construct validity of this newly adapted tool was determined by verifying the strength of correlation between the TIS-PL and the Polish version of the Fugl-Meyer Assessment Scale (FMA-PL) total and subscale scores (23). The second aim was to determine the correlation between the TIS-PL and ARAT-PL to verify the strength of the association between trunk function and upper extremity activity.
METHODS
Study design, participants, initial evaluation
In this 7-month cross-sectional study, 80 patients with stroke were recruited from the Bonifraterskie Centrum Zdrowia hospital in Piaski, Poland. The inclusion criteria were as follows: (i) a diagnosis of stroke, indicated by computed tomography scans or magnetic resonance imaging, (ii) the presence of hemiparesis, and (iii) no additional neurological or orthopaedic disabling deficits. The exclusion criteria were (i) hemiplegia in the upper extremity (assessed by a neurologist), (ii) serious visual and hearing disorders, (iii) cognitive decline that limited administration of the tests, (iv) disorders of speech and language, (v) native language other than Polish, and (vi) hip prosthesis.
The data collected in the initial evaluation included age, sex, weight, height, and upper limb dominance. Furthermore, data on time post-stroke, lesion type, lesion location, involved side of the lesion, presence of comorbidities, and duration of hospital rehabilitation were collected. Ethical approval (187/19) was obtained from the Bioethical Committee of Poznan University of Medical Sciences, and the study was conducted in accordance with the tenets of the Declaration of Helsinki. All participants provided informed consent at the time of enrolment in the study.
Outcome measures
TIS. The TIS comprises 3 subscales: Static sitting balance, Dynamic sitting balance, and Coordination. The 3 subscales comprise 3, 10, and 4 items, respectively. The scale scores range from 0 to 23, with higher scores indicating better trunk control. The total scores of the Static sitting balance, Dynamic sitting balance, and Coordination sections are 7, 10, and 6, respectively. Participants are required to maintain the sitting position for at least 10 s for testing (12).
FMA. The FMA was investigated to evaluate sensorimotor impairments in patients with stroke (24). This measure comprises 5 domains: motor functioning, balance, sensation, joint range of motion, and joint pain (24). The Polish version of FMA was used in this study (23). Only the motor domain of the Polish version of the FMA for the upper (FMA-UE-PL) and lower (FMA-LE-PL) extremities was administered (23). The motor score is expressed on a 3-point ordinal scale: 2 points indicate the task was fully performed, 1 point indicates it was partially performed, and 0 points indicate it was not performed. The maximum scores for the FM-UE and FM-LE are 66 and 34 points, respectively (25–27).
ARAT. The ARAT assesses upper-limb activity capacity according to the International Classification of Functioning, Disability and Health (ICF), specifically dexterity and object-handling abilities. The ARAT consists of 19 items across the subtests Grasp, Grip, Pinch, and Gross Movement. The subtest Grasp and Pinch comprises 6 items, each. The subtests Gross Movement and Grip comprise 3 and 4 items, respectively. The total ARAT score is the sum of the scores of 19 items. The maximum attainable score is 57 points. Each functional task is assigned an ordinal score of 0, 1, 2, or 3 points. Higher values indicate better upper limb functional status (22).
The TIS translation and cultural adaptation
The TIS was translated into Polish in accordance with international guidelines (28–31). First, we obtained permission to proceed with cultural adaptation and validation from the author of the original TIS (12). The English version of the TIS was then independently translated by 2 Polish translators fluent in English (1 specialized in the field of rehabilitation). Two Polish versions were collated; differences between the translations were discussed, corrected, and a common draft version was jointly established. In the next stage, this Polish draft was independently back-translated into English by 2 certified English translators. The common retranslated English version was then compared with the original English version by 2 physiotherapists fluent in English. Corrections were made to the retranslated version, and a panel of judges consisting of a neurologist, 2 physiotherapists specialized in neurology, 1 in clinical neurophysiology, and 1 in orthopaedics, a psychologist, and translators compared and discussed the translated and original versions of the TIS. The emerging Polish version of TIS was corrected to account for all differences, achieving a satisfactory balance between cultural language requirements and the original English scale, yielding the pre-final version of the TIS-PL. This version was then applied in a pilot study with a small group of participants and declared final.
Assessment procedure
The 2 experienced neurological physiotherapists, well trained in administering the scales, carried out the TIS-PL, FMA-UE-PL, FMA-LE-PL, and ARAT-PL. To determine test–retest reliability, the same rater examined the patients twice a day, with a 2-h gap between assessments. Inter-rater reliability was assessed by 2 observers who independently examined patients simultaneously in a silent hospital room (32). Results were collected for the total and subscale scores of the TIS-PL, FMA-PL, and ARAT-PL.
Statistical analysis
The statistical analysis was conducted using the statistical software package Statistica 13 (Tibco Software Inc, 2017, Polska, Kraków, Poland) (33) and RStudio (psych package version 2.4.3; R Foundation for Statistical Computing, Vienna, Austria) (34).
Internal consistency. Internal consistency was evaluated by calculating Cronbach’s alpha coefficients for the subscales and the total scale. The Cronbach’s alpha values indicate excellent, adequate, and poor results as above 0.80, 0.70–0.79, and below 0.70, respectively (35, 36).
Reliability. The test–retest and inter-rater reliability of the TIS-PL were estimated using Cohen’s kappa (κ), the intraclass correlation coefficient (ICC), and percentage agreement (PA). Item reliability was determined when agreement exceeded 80% (37). Cohen’s kappa values can range from 0 (no agreement) to 0.01–0.20 (none to slight), 0.21–0.40 (fair), 0.41–0.60 (moderate), 0.61–0.80 (substantial), and 0.81–1.00 (almost perfect agreement) (38). The correlation coefficients range from 0–0.30, indicating little or no correlation between the studied variables; from 0.30–0.50, indicating low correlation; from 0.50–0.70, indicating moderate correlation; from 0.70–0.90, indicating high correlation; and from 0.90–1.00, indicating very high correlation (20).
Validity. Construct validity was assessed using hypothesis testing according to the guidelines of the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) (30). A total of 8 independent hypotheses were formed. For all the hypotheses, we defined the correlation direction, the correlation strength (calculated as the Spearman rank correlation coefficient, rho), and the rationale for each (Tables I and II). The relationships among TIS-PL, FMA-UE-PL, and ARAT-PL scores (4 hypotheses for each) and FMA-LE-PL scores (4 hypotheses) were examined to estimate the extent to which the observed correlations are consistent with the formulated hypotheses. The TIS-PL construct validity rating was determined according to the total number of confirmed hypotheses; 6–8 (≥ 75%) confirmed hypotheses indicated high construct validity, while 4–5 (50% ≥) indicated moderate (30).
Relationship between trunk and upper extremity. According to the literature (4, 10, 11, 39–42), there is a link between trunk and upper extremity function. Thus, we hypothesized that a significant correlation between the TIS and the ARAT would be present. This correlation was evaluated by calculating Spearman’s rank correlation coefficients for the relationship between the ARAT-PL (43) and the TIS-PL. Correlation is considered low when the calculated coefficient is between 0.30 and 0.50, moderate when it is between 0.50 and 0.70, high when it is between 0.70 and 0.90, and very high when it is between 0.90 and −1.00 (44).
Floor and ceiling effects. Floor and ceiling effects were established as the percentages of participants who scored beyond the lower (floor) and upper (ceiling) boundaries of the total TIS-PL score (0–23).
The cut-off points for these boundaries were set at 5%. Therefore, scores under 1 were determined as the floor, while those above 22 were considered ceiling effects. Floor and ceiling effects were considered significant if more than 20% of the participants fell outside the set lower or upper boundaries, respectively (45).
RESULTS
Patients’ clinical characteristics
Eighty patients with subacute and chronic stages of stroke participated in the examination. The patient demographics are presented in Table III.
Translation and cultural adaptation
Forward, backward, and final versions of the translation. Several linguistic differences were detected during the first review of the Polish version of TIS translated from English. These differences mainly concerned contextual variations in the clarification or manner of expressing concepts. With few exceptions, Polish is characterized by a more long-winded style of expression and is richer in words with variable, very specific meanings. Therefore, the concise or slender English phrases or sentences were supplemented or replaced with more detailed and elaborated Polish ones. Some discrepancies were found when the original version was compared with the common version resulting from 2 back translations. As expected, all words added in the Polish version during forward translation were also added in the back translation. During the panel meeting, all versions of the survey were compared; whenever any language doubt arose, specific stylistic corrections were made, and sentences were rephrased to make the text more comprehensible to general respondents (Table IV).
Reliability
The mean scores of the TIS-PL, FMA-UE-PL, and FMA-LE-PL obtained from the participants are presented in Table V. Differences in scores between raters for each TIS-PL assessment are presented in Table VI.
Internal consistency. The TIS-PL total score demonstrated excellent internal consistency (Cronbach’s alpha = 0.89). Equivalently, Cronbach’s α values for the subscale scores were excellent (α = 0.85–0.91).
Test–retest. The test–retest reliability, as measured by kappa values, for the TIS-PL items’ scores was almost perfect (Table VII). The ICC (2,k) values determined for each subscale and the total score ranged from 0.94 to 1.00, showing excellent reliability (Table VIII).
Inter-rater. The TIS-PL subscale items exhibited moderate to almost perfect κ values, ranging from 0.66 to 1.0 (Table VII). The ICC (2,k) values for each subscale and the total instrument score ranged from 0.81 to 0.99, indicating good to excellent reliability (Table IX).
Validity
The relationships between the scores of the TIS-PL, FMA-UE-PL, and FMA-LE-PL are presented in Fig. 1A, B. High correlations were found between the TIS-PL and FMA-UE-PL (rho = 0.71) total scores and the TIS-PL and FMA-LE-PL (rho = 0.76) total scores (see Tables I and II). Similarly, the correlations between the Dynamic sitting balance subscale score and the FMA-UE-PL total score, as well as between the Coordination subscale score and the FMA-LE-PL total score, were high. Moderate correlations were found between the Coordination subscale score and the FMA-UE-PL total score, as well as between the Dynamic sitting balance subscale score and the FMA-LE-PL total score. The correlations between the Static sitting balance subscale score and the FMA-UE-PL and FMA-LE-PL total scores were low. Based on the absolute scoring method, 6 out of 8 hypotheses for the TIS-PL were confirmed (75%), indicating moderate construct validity (Tables I and II).
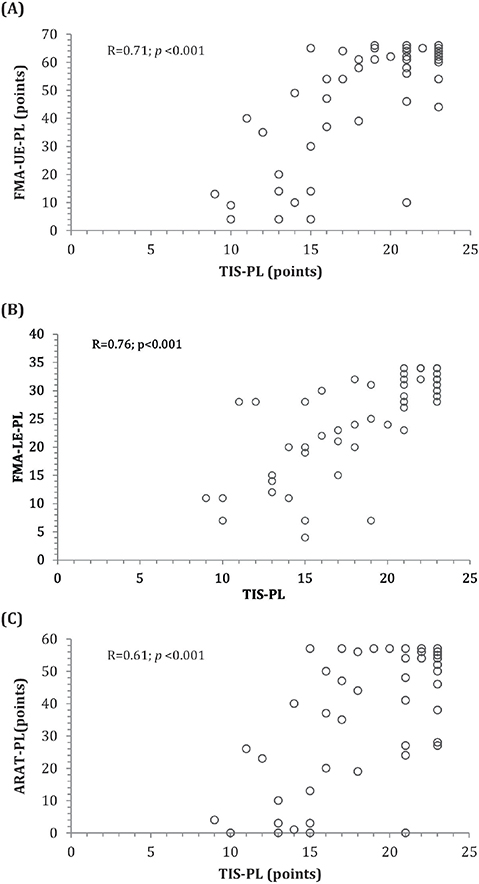
Fig. 1. Relationship between (A) the TIS-PL and FMA-UE scores, (B) the TIS-PL and FMA-LE scores, and (C) the TIS-PL and ARAT-PL scores.
The relationships between the TIS-PL and ARAT-PL scores are presented in Fig. 1C. The correlation between the TIS-PL and the ARAT-PL for absolute scores was moderate (rho = 0.61). A low-to-high correlation was observed between the TIS-PL and ARAT-PL subscale scores (Table X).
Floor and ceiling effects
The TIS-PL showed a significant ceiling effect, affecting 46% of the participants evaluated. No floor effect was detected (0%).
DISCUSSION
The purpose of this study was to determine the reliability and validity of the culturally adapted Polish version of the TIS. The results indicated that the TIS-PL demonstrated moderate to excellent reliability and moderate construct validity. Additionally, a moderate relationship was generally observed between trunk function, as assessed by the TIS-PL, and upper extremity activity, as measured by the ARAT-PL, in individuals after stroke. However, high positive correlations were observed between dynamic trunk postural control and fine motor skills of the hand and fingers in stroke patients.
Reliability
In this study, excellent test–retest reliability was found for the total and subscale scores TIS-PL. Similar results have been reported in the literature by Verheyden et al. (12) and Sağ (17), who presented ICC coefficients ranging from 0.96 to 1 for the test–retest reliability of this instrument. Other studies (13, 15, 16) have demonstrated good to high test–retest reliability indices, ranging from 0.67 to 0.98, as assessed by Cohen’s kappa coefficients. The inter-rater reliability of the TIS-PL as per Cohen’s kappa coefficient and the ICC was perfect. The degree of agreement among independent raters was moderate for 2 items and good for 1 item. The inter-rater reliability scores from previous studies vary widely, from 0.49 to 0.99 (қ, ICC) (13, 15, 16). However, excellent inter-rater reliability has been reported for the original version of the scale (12).
The Cohen’s kappa coefficient indicated an almost perfect level of agreement, and the interobserver agreement, measured via percentage agreement, was ≥0.90. Thus, the results provide evidence that the Polish version of the TIS demonstrates moderate to excellent reliability, comparable to that of the original version. Moreover, our findings appear robust, as all previous studies included substantially smaller sample sizes than ours.
Internal consistency
The total and subscale scores of the TIS-PL presented excellent internal consistency. The Cronbach’s alpha values for the Static sitting balance, Dynamic sitting balance, Coordination, and total TIS-PL scores were 0.90, 0.85, 0.91, and 0.89, respectively. These results are consistent with those reported in previous studies, which ranged from α = 0.61 to 0.97 (12, 13, 15, 16). Our findings indicate that the Polish version of TIS has been accurately translated and exhibits consistency comparable to the original scale. Notably, for the Coordination subscale, the TIS-PL results showed slightly higher internal consistency than the original version reported by Verheyden et al. (12).
Validity
The construct validity of the TIS-PL was established. Correlation coefficients were calculated for TIS-PL, FMA-UE-PL, and FMA-LE-PL. High correlation was observed between the total scores of the scales, with coefficients of 0.71 and 0.76, respectively. However, different patterns emerged across the subscales. Correlations between the TIS-PL subtests and FMA-UE-PL ranged from low to high (R = 0.42 to 0.72). A slightly lower correlation was found between the TIS-PL subtests and FMA-LE-PL, indicating low to moderate relationships (R = 0.39–0.69). Our findings suggest that the strongest correlation was observed with lower extremity function, while correlations with upper extremity function were slightly weaker. After analysing all the predefined hypotheses, the TIS-PL demonstrated moderate construct validity. Our choice of comparator tools was guided by the functional relationship between trunk and limb movement (4, 19, 20, 39, 40, 42–47) and the availability of a validated Polish version of the outcome measure. To our knowledge, the construct validity of the TIS has been tested using hypothesis-driven methods in only 1 other study (48). That study reported acceptable correlations (R > 0.4) using Pearson’s coefficients between the TIS and the Barthel Index, the Trunk Control Test, and the Functional Independence Measure. Another study (1) reported good construct validity; however, a different method – Confirmatory Factor Analyses – was employed.
Relationship between trunk function and upper extremity activity
The strength of the correlation between the TIS-PL and ARAT-PL scores was calculated. According to the literature, there is a relationship between the level of trunk postural control and upper extremity functional activity in patients after stroke. In this study, high to moderate positive correlations were found between the total and partial scores of the TIS-PL and ARAT-PL assessments. In a few cases, low positive correlations were observed between specific subscale scores of the 2 outcome measures. A high correlation was found between the Dynamic sitting balance subscale of the TIS-PL and the Grasp, Grip, and Global movement subtests of the ARAT-PL (rho = 0.75, 0.73, and 0.72, respectively). Moderate correlations (rho = 0.50–0.57) were observed between the Coordination subscale of the TIS-PL and all ARAT-PL subtests. The lowest correlations (rho = 0.38–0.50) were observed for the Static sitting balance subscale, indicating weak relationships.
To our knowledge, no previous study has reported a correlation between upper-extremity activity assessed with the ARAT and trunk postural control assessed with the TIS. In addition, the literature does not present such detailed analyses of correlation relationships between the results of individual subtests of both outcome measures. The relationship between the level of impairment in the upper extremity and trunk in stroke was presented by Likhi et al. (4). Trunk control was evaluated using the TIS, and upper extremity functional performance was evaluated using the Simplified Stroke Rehabilitation Assessment of Movement. A lower correlation was observed than that in this study (rho = 0.50-0.60). Another study compared the results of the TIS and the FMA-UE. A moderate relationship (rho = 0.53, rho = 0.67) was found between the results obtained in these assessments (37, 38). In this case, the tested compound was at a lower level than ours. Thus, the results presented in this work indicate a stronger relationship between individual trunk control skills and various upper extremity functional skills in stroke than has been shown in previous studies. In particular, the results of the TIS-PL dynamic sitting balance subtest are highly correlated with the ability to perform various types of grips. This demonstrates a strong connection between upper-limb gross and fine motor control and trunk posture control in the sitting position in people with stroke. Moreover, a high correlation was observed between contralateral trunk movements and upper-limb function. This may indicate a relationship between the degree of trunk muscle tension on one side and the functional efficiency of the upper limb (gripping and manipulating the hand) on the opposite side. Although one of the conditions for standardizing measurements during the ARAT test was to maintain the trunk resting on the chair, the present study found that trunk control is essential when using the upper extremities, even in a propped position.
Trunk control provides the fundamental proximal stability required for efficient and coordinated upper limb movements. Furthermore, stronger trunk function is associated with better upper limb performance and recovery in both healthy individuals and stroke survivors (41–45).
Floor and ceiling effect
No floor effect was observed in our study; however, a significant ceiling effect was present, affecting 46% of participants. These findings suggest that a substantial proportion of the participants experienced little difficulty in completing the tasks. The Coordination subscale was the only component that posed greater demands on the participants. It appears that TIS-PL is an outcome measure that may not effectively differentiate patients with minimal trunk impairment and is more suitable for assessing individuals with moderate to severe trunk dysfunction. This observation may indicate that, for some subscales, the TIS scoring system is not sufficiently sensitive to detect subtle deficits in patients who have largely recovered after a stroke or who exhibit mild trunk impairment.
Strengths of the study
The present study provides the first validated Polish version of a standardized tool for assessing trunk control after stroke, addressing a gap in Polish neurorehabilitation research and practice. The translation and cross-cultural adaptation followed international guidelines, ensuring conceptual and linguistic accuracy. Psychometric testing demonstrated excellent reliability and moderate validity, confirming that the scale is both consistent and clinically relevant. Moreover, the instrument is brief and practical, making it feasible for routine clinical and research use.
Limitations
This study has several limitations. First, although the sample size was adequate for preliminary validation, it was relatively small and limited to a single clinical population, potentially limiting generalizability. Second, the study did not include a longitudinal assessment to evaluate responsiveness or sensitivity to change over time. Third, the sample was heterogeneous in terms of the type of rehabilitation participants were undergoing. Moreover, many patients demonstrated a relatively high level of functional control of the trunk and upper limbs, resulting in a ceiling effect. This likely restricted score variability, reduced measurement error, and inflated both intra- and inter-rater reliability estimates. Consequently, this exaggerated reliability may also have affected our validity measures, as the TIS failed to discriminate between many individuals. Future research should therefore include individuals with moderate and low levels of motor impairment following stroke to better evaluate the discriminatory power of the TIS-PL. Additionally, the relevance of this research is currently restricted to the Polish population, and comparable studies are recommended for other nations. Finally, the lack of a culturally adapted Polish version of a trunk control scale represents a methodological limitation; however, the use of the ARAT and FMA was reasonable given the instrument’s unavailability.
Conclusion
The Polish version of the TIS-PL demonstrates almost perfect reliability and moderate construct validity. Our results support the clinical and research use of the TIS-PL as a valid outcome measure for assessing trunk impairment in the Polish post-stroke population. Furthermore, the novel finding is that a higher level of dynamic trunk postural control is associated with greater fine motor skills of the hand and fingers in stroke patients.
REFERENCES
- Gjelsvik B, Breivik K, Verheyden G, Smedal T, Hofstad H, Strand LI. The Trunk Impairment Scale modified to ordinal scales in the Norwegian version. Disabil Rehabil 2012; 34: 1385–1395. https://doi.org/10.3109/09638288.2011.645113
- Kılınç M, Avcu F, Onursal O, Ayvat E, Savcun Demirci C, Aksu Yildirim S. The effects of Bobath-based trunk exercises on trunk control, functional capacity, balance, and gait: a pilot randomized controlled trial. Top Stroke Rehabil 2016; 23: 50–58. https://doi.org/10.1179/1945511915Y.0000000011
- Verheyden G, Vereeck L, Truijen S, Troch M, Herregodts I, Lafosse C, et al. Trunk performance after stroke and the relationship with balance, gait and functional ability. Clin Rehabil 2006; 20: 451–458. https://doi.org/10.1191/0269215505cr955oa
- Likhi M, Jidesh Vv, Kanagaraj R, George JK. Does trunk, arm, or leg control correlate best with overall function in stroke subjects? Top Stroke Rehabil 2013; 20: 62–67. https://doi.org/10.1310/tsr2001-62
- Bohannon RW, Leary KM. Standing balance and function over the course of acute rehabilitation. Arch Phys Med Rehabil 1995; 76: 994–996. https://doi.org/10.1016/s0003-9993(95)81035-8
- Büyükavcı R, Şahin F, Sağ S, Doğu B, Kuran KB. The impact of additional trunk balance exercises on balance, functional condition and ambulation in early stroke patients: randomized controlled trial. Turk J Phys Med Rehab 2016; 62: 248–256. https://doi.org/10.5606/tftrd.2016.84770
- Cabanas-Valdes R, Cuchi GU, Bagur-Calafat C. Trunk training exercises approaches for improving trunk performance and functional sitting balance in patients with stroke: a systematic review. NeuroRehabilitation 2013; 33: 575–592. https://doi.org/10.3233/NRE-130996
- Shin JW, Kim KD. The effect of enhanced trunk control on balance and falls through bilateral upper extremity exercises among chronic stroke patients in a standing position. J Phys Ther Sci 2016; 28: 194–197. https://doi.org/10.1589/jpts.28.194
- Wee SK, Hughes AM, Warner MB, Brown S, Cranny A, Mazomenos EB, et al. Effect of trunk support on upper extremity function in people with chronic stroke and people who are healthy. Phys Ther 2015; 95:1163–1171. https://doi.org/10.2522/ptj.20140487
- Verheyden G, Nieuwboer A, de Wit L, Thijs V, Dobbelaere J, Devos H, et al. Time course of trunk, arm, leg, and functional recovery after ischemic stroke. Neurorehabil Neural Repair 2008; 22: 173–179. https://doi.org/10.1177/1545968307305456
- Lee KB, Lim SH, Kim KH, Kim KJ, Kim YR, Chang WN, et al. Six-month functional recovery of stroke patients: a multi-time-point study. Int J Rehabil Res 2015; 38: 173–180. https://doi.org/10.1097/MRR.0000000000000108
- Verheyden G, Nieuwboer A, Mertin J, Preger R, Kiekens C, de Weerdt W. The Trunk Impairment Scale: a new tool to measure motor impairment of the trunk after stroke. Clin Rehabil 2004; 18: 326–334. https://doi.org/10.1191/0269215504cr733oa
- Seo HD, Kim NJ, Chung YJ. Reliability of the Korean Version of the Trunk Impairment Scale in patients with stroke. Phys Ther Korea 2008; 15: 87–96.
- Castellassi CS, Ribeiro EAF, Fonseca VC, Beinotti F, Oberg TD, Lima NMF. Reliability of Brazilian version trunk impairment scale for stroke patients [Portuguese]. Fisioter Mov 2009; 20: 114–125.
- Cabanas-Valdés R, Urrútia G, Bagur-Calafat C, Caballero-Gómez FM, Germán-Romero A, Girabent-Farrés M. Validation of the Spanish version of the Trunk Impairment Scale Version 2.0 (TIS 2.0) to assess dynamic sitting balance and coordination in post-stroke adult patients. Top Stroke Rehabil 2016; 23: 225–232. https://doi.org/10.1080/10749357.2016.1151662
- Lombardi B, Orioli A, Casavola D, Paci M. The Italian version of the Trunk Impairment Scale: development and psychometric properties. Eur J Phys Rehabil Med 2017; 53: 516–520. https://doi.org/10.23736/S1973-9087.17.04371-4
- Sağ S. The validity and reliability of the Turkish Version of the Trunk Impairment Scale in stroke patients. North Clin Istanb 2018; 6: 156–165. https://doi.org/10.14744/nci.2018.01069
- Fujiwara T, Liu M, Tsuji T, Sonoda S, Mizuno K, Akaboshi K, et al. Development of a new measure to assess trunk impairment after stroke (Trunk Impairment Scale): its psychometric properties. Am J Phys Med Rehabil 2004; 83: 681–688. https://doi.org/10.1097/01.PHM.0000137308.10562.20
- Bernstein I, Nunnally J. Psychometric theory. 3rd ed. New York: McGraw-Hill; 1994.
- Hinkle DE, Wiersma W, Jurs SG. Applied statistics for the behavioral sciences. 2nd ed. Boston: Houghton Mifflin; 1988.
- Alhwoaimel N, Turk R, Warner M, Verheyden G, Thijs L, Wee SK, et al. Do trunk exercises improve trunk and upper extremity performance, post stroke? A systematic review and meta-analysis. NeuroRehabilitation 2019; 43: 95–412. https://doi.org/10.3233/NRE-182446
- Yozbatiran N, Der-Yeghiaian L, Cramer SC. A standardized approach to performing the action research arm test. Neurorehabil Neural Repair 2008; 22: 78–90. https://doi.org/10.1177/1545968307305353
- Goliwas M, Malecka J, Adamczewska K, Flis-Maslowska M, Lewandowski J, Kocur P. Polish cultural adaptation and reliability of the Fugl-Meyer Assessment of Motor Performance and Sensory Assessment Scale in stroke patients. J Clin Med 2024; 13: 3710. https://doi.org/10.3390/jcm13133710
- Cecchi F, Carrabba C, Bertolucci F, Castagnoli C, Falsini C, Gnetti B, et al. Transcultural translation and validation of Fugl-Meyer assessment to Italian. Disabil Rehabil 2021; 43: 3717–3722. https://doi.org/10.1080/09638288.2020.1746844
- Fugl-Meyer AR, Jääskö L, Leyman I, Olsson S, Steglind S. The post-stroke hemiplegic patient 1. A method for evaluation of physical performance. Scand J Rehabil Med 1975; 7: 13–31.
- Page SJ, Hade E, Persch A. Psychometrics of the wrist stability and hand mobility subscales of the Fugl-Meyer Assessment in moderately impaired stroke. Phys Ther 2015; 95: 103–108. https://doi.org/10.2522/ptj.20130235
- Gladstone DJ, Danells CJ, Black SE. The Fugl-Meyer Assessment of motor recovery after stroke: a critical review of its measurement properties. Neurorehabil Neural Repair 2002; 16: 232–240. https://doi.org/10.1177/154596802401105171
- Guillemin F, Bombardier C, Beaton D. Cross-cultural adaptation of health-related quality of life measures: literature review and proposed guidelines. J Clin Epidemiol 1993; 46: 1417–1432. https://doi.org/10.1016/0895-4356(93)90142-N
- Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine (Phila Pa 1976) 2000; 25: 3186–3191. https://doi.org/10.1097/00007632-200012150-00014
- Mokkink LB, Prinsen CA, Donald PL, Alonso J, Bouter LM, de Vet HC, et al. COSMIN methodology for systematic reviews of Patient-Reported Outcome Measures (PROMs). VU Univ Med Cent 2018; 27: 1147–1157.
- Szczechowicz J, Lewandowski J, Sikorski J. Polish adaptation and validation of Burn Specific Health Scale - Brief. Burns 2014; 40: 1013–1018. https://doi.org/10.1016/j.burns.2013.11.026
- Mokkink LB, Terwee CB, Patrick DL, Alonso J, Stratford PW, Knol DL, et al. The COSMIN study reached international consensus on taxonomy, terminology, and definitions of measurement properties for health-related patient-reported outcomes. J Clin Epidemiol 2010; 63: 737–745. https://doi.org/10.1016/j.jclinepi.2010.02.006
- TIBCO Software Inc. Statistica (data analysis software system), version 13. 2017. Available from: http://statistica.io
- Revelle W. psych: Procedures for Psychological, Psychometric, and Personality Research. Version 2.1.3. Northwestern University; 2021. Available from: https://CRAN.R-project.org/package=psych
- Andresen EM. Criteria for assessing the tools of disability outcomes research. Arch Phys Med Rehabil 2000; 81: S15–20. https://doi.org/10.1053/apmr.2000.20619
- Bernstein I, Nunnally J. Psychometric theory, 3rd ed. New York: McGraw-Hill; 1994.
- McHugh ML. Interrater reliability: the kappa statistic. Biochem Med (Zagreb) 2012; 22: 276–282. https://doi.org/10.11613/bm.2012.031
- Barreca, S, Stratford, PW, Lambert, CL, Masters, LM, Streiner, DL. Test–retest reliability, validity, and sensitivity of the Chedoke Arm and Hand Activity Inventory: a new measure of upper-limb function for survivors of stroke. Arch Phys Med Rehabil 2005; 86: 1616–1622. https://doi.org/10.1016/j.apmr.2005.03.017
- Duncan PW, Goldstein LB, Horner RD, Landsman PB, Samsa GP, Matchar DB. Similar motor recovery of upper and lower extremities after stroke. Stroke 1994; 25: 1181–1188.
- Wee SK, Hughes AM, Warner MB, Brown S, Cranny A, Mazomenos EB, et al. Effect of trunk support on upper extremity function in people with chronic stroke and people who are healthy. Phys Ther 2015; 95: 1163–1171. https://doi.org/10.2522/ptj.20140487
- Akkurt L, Yağcıoğlu GA, Aksoy CC, Yaman F. The effect of trunk control on sitting balance and upper extremity functions in patients with subacute stroke. Neurological Sciences 2024; 45: 5807–5812. https://doi.org/10.1007/s10072-024-07817-w
- Okada T, Huxel Bliven KC, McMullen J. Relationship between core stability, functional movement, and performance. J Strength Cond Res 2011; 25: 252–261. https://doi.org/10.1007/s10072-024-07817-w
- Karthikbabu S, Chakrapani M, Ganeshan S, Rakshith, KC, Nafeez S, Prem V. A review on assessment and treatment of the trunk in stroke: A need or luxury? Disabil Rehabil 2012; 33: 2119–2126. https://doi.org/10.3109/09638288.2011.574776
- Shumway-Cook A, Woollacott H. Motor control. 5th ed. Philadelphia: Wolters Kluwer; 2017. p. 183–305.
- Robertson J, Roby-Brami A. The trunk as a part of the kinematic chain for reaching movements in healthy subjects and hemiparetic patients. Brain Res 2011; 1382: 137–146. http://doi.org/10.1016/j.brainres.2011.01.043
- Małecka J, Goliwąs M, Adamczewska K, Lewandowski J, Łochyński D. The translation into Polish, cultural adaptation, and initial validation of the Action Research Arm Test in subacute stroke patients. Adv Clin Exp Med 2025; 34: 1165–1173. https://doi.org/10.17219/acem/191775
- Likhi M, Jidesh VV, Kanagaraj R, George JK. Does trunk, arm, or leg control correlate best with overall function in stroke subjects? Top Stroke Rehabil 2013; 20: 62–67. https://doi.org/10.1310/tsr2001-62
- Monticone M, Ambrosini E, Verheyden G, Brivio F, Brunati R, Longoni L, et al. Development of the Italian version of the trunk impairment scale in subjects with acute and chronic stroke. Cross-cultural adaptation, reliability, validity and responsiveness. Disabil Rehabil 2019; 41: 66–73. https://doi.org/10.1080/09638288.2017.1373409