ORIGINAL REPORT
LATENT PROFILE ANALYSIS OF SOCIAL PARTICIPATION IN STROKE SURVIVORS WITH LIMB DYSFUNCTION: A MIXED-METHODS STUDY
Xuan ZHOU1  , Ying WANG2 and Lanshu ZHOU1
, Ying WANG2 and Lanshu ZHOU1
From the 1School of Nursing, Naval Medical University, Shanghai, and 2Department of Nursing, Shanghai First Rehabilitation Hospital, Shanghai, China
Objective: This study aimed to identify profiles of social participation among stroke survivors with limb dysfunction and explore the factors influencing these profiles.
Design: A convergent mixed-methods design.
Methods: The quantitative phase involved 499 participants recruited from 5 neurorehabilitation centres in Shanghai between December 2023 and June 2025. Participants completed measures including the Utrecht Scale for Evaluation of Rehabilitation-Participation (USER-P), the Connor-Davidson Resilience Scale (CD-RISC-10), and the Modified Rankin Scale (mRS). Qualitative semi-structured interviews were performed with 16 participants to explore lived experiences of social participation.
Results: Latent profile analysis revealed 4 distinct social participation profiles: “Active Integration”, “Contented Conservatism”, “Cautious Conservatism”, and “Alienated Disengagement”. A multivariate analysis identified age, resilience, and physical function as significant predictors of profile membership. Qualitative findings uncovered 2 core emotional experiences (a sense of loss vs a sense of rebuilding) and 3 behavioural patterns (activist, conservative, alienated), which effectively explained the quantitative profiles’ characteristics and their underlying mechanisms. The integration of data provided a nuanced person-centred framework depicting the heterogeneity in post-stroke social participation.
Conclusion: Social participation among stroke survivors is heterogeneous and can be classified into 4 distinct profiles shaped by the interplay of physical function, resilience, and sociodemographic factors. The findings underscore the necessity of implementing profile-specific, stepped-care interventions for effectively enhancing post-stroke social participation.
LAY ABSTRACT
Stroke often causes extremity disability, significantly impacting survivors’ ability to engage in social activities. This study aimed to understand the different ways stroke survivors participated in society. We surveyed 499 stroke survivors and interviewed 16 others. We identified 4 distinct patterns: “Active Integration” (actively engaged), “Contented Conservatism” (less active but satisfied), “Cautious Conservatism” (less active and dissatisfied), and “Alienated Disengagement” (largely withdrawn). The pattern a stroke survivor fell into was influenced not just by physical function but also by age, psychological resilience, and emotional outlook – particularly whether they focused on loss or on rebuilding their life after stroke. These findings highlight that personalized support plans, tailored to an individual’s specific needs and mindset, are crucial for effectively helping stroke survivors regain social connection and improve their quality of life.
Key words: stroke; social participation; latent profile analysis; mixed-methods study; limb dysfunction.
Citation: J Rehabil Med 2026; 58: jrm44832. DOI: https://doi.org/10.2340/jrm.v58.44832.
Copyright: © 2026 The Author(s). Published by MJS Publishing, on behalf of the Foundation for Rehabilitation Information. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/).
Submitted: Sept 23, 2025; Accepted after revision: Nov 6, 2025; Published: Jan 7, 2026.
Correspondence address: Ying Wang, Department of Nursing, Shanghai First Rehabilitation Hospital, 349 Hangzhou Road, Yangpu District, Shanghai, 200090, China, and Lanshu Zhou, School of Nursing, Naval Medical University, 800 Xiangyin Road, Yangpu District, Shanghai 200433, China. E-mail: 114404394@qq.com; zhoulanshu@hotmail.com
Competing interests and funding: The authors have no conflicts of interest to declare.
This work was supported by the National Natural Science Foundation of China [82202816].
Stroke is a leading cause of long-term disability worldwide, affecting millions of people each year. According to the World Health Organization, there are over 12 million new cases of stroke annually (1). In China, the disease burden is substantial, with an estimated 17.8 million stroke survivors, 3.4 million new cases, and 2.3 million deaths in 2020 (2). Furthermore, approximately 12.5% of stroke survivors were left with significant disability. These conditions, particularly limb dysfunction, profoundly impact patients’ social participation and quality of life (3). Social participation, which encompasses roles, activities, and interpersonal connections, is a critical determinant of post-stroke recovery and psychosocial well-being (4, 5). However, stroke survivors frequently face multifaceted challenges in social reintegration (6), which can further hinder physical recovery, exacerbate psychological distress, and increase mortality risk (7, 8).
Existing evidence suggests that social participation in stroke survivors is influenced by a complex interplay of factors, including mobility limitations, resilience, and environmental barriers (9–11). Despite this understanding, interventions targeting these factors, such as exercise-based programmes, self-management strategies, and occupational therapy, have yielded inconsistent outcomes in improving social participation (12, 13). This discrepancy may stem from the heterogeneous nature of post-stroke social participation patterns, which are often overlooked in standardized, one-size-fits-all intervention approaches. A paradigm shift towards individualized strategies that are tailored to distinct participation profiles is urgently needed (14).
To address this gap, our study employs a convergent mixed-methods design to provide a comprehensive understanding of this heterogeneity. This approach integrates: (i) latent profile analysis (LPA), a person-centred statistical approach that identifies homogeneous subgroups within heterogeneous populations based on social participation metrics (frequency, restrictions, and satisfaction); and (ii) qualitative thematic analysis, which captures the lived experiences and emotional responses that quantitative tools cannot fully elucidate (15, 16). Through this dual-focus lens, this study aims to identify latent profiles of social participation among stroke patients with limb dysfunction and examine potential factors associated with distinct participation profiles.
METHODS
This study adopted a convergent mixed-methods design to comprehensively explore the profiles of social participation. This approach allowed for the triangulation of quantitative patterns with qualitative experiences, providing a more complete understanding, though it also presented challenges in data integration. The study was conducted in accordance with the Declaration of Helsinki, with the protocol receiving ethical approval from the Ethics Committee of Shanghai First Rehabilitation Hospital (2022-01-001). Written informed consent was obtained from all study participants. This study adheres to the Reporting Guidelines for Mixed Methods Research in Rehabilitation Health Sciences (17).
Participants
Participants were recruited from 5 neurorehabilitation departments in Shanghai, China, between December 2023 and June 2025. The inclusion criteria were defined as follows: (i) diagnosis of stroke confirmed by CT or MRI; (ii) age ≥18 years old; (iii) stable vital signs and absence of other serious comorbidities, such as cancer or organ failure; (iv) disease duration of at least 3 months; (v) presence of limb dysfunction with a modified Rankin Scale (mRS) score between 1 and 4; and (vi) voluntary participation in this study. Exclusion criteria included: (i) language communication disorders; (ii) cognitive impairment, defined as a Montreal Cognitive Assessment (MoCA) score < 26; and (iii) severe emotional disorders. Based on methodological recommendations that latent profile analysis (LPA) requires a sample size between 300 and 500 (18), a total of 499 stroke survivors successfully completed the survey, yielding an effective response rate of 92.1%. For the qualitative phase, participants were selected based on the same eligibility criteria using a purposive sampling strategy. Between March 2025 and June 2025, stroke patients were recruited from both neurorehabilitation departments and community settings. The sampling aimed to maximize variation across key characteristics such as age, educational background, and disease course. Data saturation was determined to be achieved after the 16th interview, at which point no new themes emerged.
Measurements
Data on sociodemographic and clinical characteristics were collected using a purpose-designed questionnaire, including age, gender, educational level, stroke type, and time after onset.
Social participation was assessed using the Utrecht Scale for Evaluation of Rehabilitation-Participation (USER-P), which comprises 32 items across 3 subscales: Participation Frequency, Participation Restriction, and Participation Satisfaction (19). The Frequency subscale contains 2 parts: 4 items rated from 0 (never) to 5 (≥36 h/week) and 7 items rated 0 (never) to 5 (≥19 times/month). The Restriction subscale includes 11 items scored from 0 (impossible) to 3 (no difficulty), and the Satisfaction subscale consists of 10 items rated 0 (very dissatisfied) to 4 (very satisfied). The USER-P does not yield a total score; instead, raw scores for each subscale are converted to a normalized score ranging from 0 to 100 using specific algorithms. Higher scores indicate higher social participation frequency, fewer participation restrictions, and greater satisfaction with participation (20). The Chinese version shows good reliability (Cronbach’s α: 0.704–0.861; test–retest: 0.734–0.832) and validity (21).
The 10-item Connor–Davidson Resilience Scale (CD-RISC-10) was utilized to evaluate the resilience level of stroke patients. Originally developed by Connor and Davidson in 2003 (22), the scale comprised 25 items distributed across 5 dimensions. Subsequently, Campbell-Sills and Stein refined it into a condensed 10-item version in 2007, enhancing its conciseness and user-friendliness. The CD-RISC-10 employs a 4-point Likert response format, ranging from 1 (not true at all) to 4 (true nearly all the time), yielding a total score that spans from 10 to 40. Higher total scores are indicative of a greater degree of resilience (23). The CD-RISC-10 exhibits strong psychometric properties, including a Cronbach’s α coefficient of 0.94, a split-half reliability coefficient of 0.89, and item-total correlations varying between 0.74 and 0.81 (23, 24).
Functional status was assessed using the mRS. The mRS was initially developed by Rankin in 1957 and was later modified and optimized by Warlow in 1988 to improve its comprehensiveness; this revised version is now the standard tool employed in clinical practice (25). The mRS utilizes a 7-level scoring system to evaluate functional independence in stroke patients, with specific criteria for each grade: a score of 0 denotes no symptoms; 1 indicates no significant disability despite symptoms; 2 corresponds to slight disability; 3 represents moderate disability; 4 indicates moderately severe disability; 5 reflects severe disability; and 6 signifies death.
Data collection
Quantitative data collection. Printed advertisements outlining the research project were distributed across 5 neurorehabilitation facilities and 1 community setting to invite eligible stroke patients to participate. All prospective volunteers were provided with comprehensive explanations regarding the study’s purpose, potential benefits, and possible risks. Each candidate was explicitly advised of their rights and responsibilities, including the unconditional right to withdraw at any time without impact on their medical care. Formal written consent was obtained from every participant prior to inclusion. Questionnaires were administered face-to-face using both paper-based forms and digital platforms such as Questionnaire Star. Before distribution, researchers clearly explained the instructions and key points for completion. After participants finished, each questionnaire was reviewed for missing responses. Where omissions were identified, the reasons were explored, and researchers provided assistance to complete any unfinished items when appropriate. For those with visual impairments or limited literacy, items were read aloud and responses were recorded on their behalf based on their verbal answers. A supportive rapport was maintained with all participants throughout the process, and contact information was gathered to enable future follow-up. A total of 545 individuals participated in the survey. Among them, 18 were excluded due to patterned responding, 26 were omitted for extensive missing data, and 2 voluntarily withdrew during the process, resulting in 499 valid responses.
Qualitative data collection. The qualitative phase employed one-on-one, in-depth, semi-structured interviews. The participants for this phase were a distinct group, separately recruited and not involved in the prior quantitative survey. This approach facilitated face-to-face dialogue between the researcher and participant, aimed at garnering rich insights into individuals’ experiences, emotions, and perspectives regarding social participation after stroke. An interview guide was developed in advance to ensure coverage of key topics while allowing flexibility to adapt to the flow of conversation. Participants were also encouraged to introduce relevant issues or questions they deemed important. Key interview topics included: current well-being; personal reflections on the stroke event; modes and extent of social participation; emotional and experiential dimensions of participation; and perceived strategies to enhance social engagement. Each interview lasted approximately 40 to 60 min to balance depth of content with participant comfort.
Data analysis
Quantitative data analysis. Statistical analyses were conducted using Mplus 8.0 (https://www.statmodel.com/) and SPSS 27.0 (IBM Corp, Armonk, NY, USA). Categorical data are presented as frequencies and percentages, while continuous data are summarized as mean and standard deviation for normally distributed variables or median and interquartile range for non-normally distributed variables. LPA was performed in Mplus 7.4 to identify subtypes of social participation among stroke patients with limb dysfunction, using the mean scores of the 3 USER-P subscales as manifest variables. The analysis commenced with a one-profile model and progressively increased the number of profiles. Model selection was guided by fit indices, including information criteria (AIC, BIC, and aBIC; lower values indicate better fit), likelihood ratio tests (LMRT and BLRT; p < 0.05 suggests significant improvement over the previous model), and entropy (range 0–1; higher values indicate clearer classification). The resulting profiles were interpreted and named based on their distinctive characteristics. Pairwise comparisons of the 3 subscales across profiles were conducted using the Kruskal–Wallis H test. The profiles were then treated as a dependent variable in univariate analyses involving χ2 and t-tests to examine associations with potential predictors. Variables that reached statistical significance (p < 0.05) in univariate analyses were entered as independent variables into a multinomial logistic regression model. A two-tailed p-value < 0.05 was considered statistically significant throughout.
Qualitative data analysis. To avoid potential bias from quantitative results, qualitative themes were extracted first. Interviews were transcribed verbatim within 24 h and verified by 2 researchers to ensure accuracy. Transcriptions adhered to principles of completeness, timeliness, and multiple backups. Nonverbal behaviours such as pauses, emotional expressions, and body language were documented in memos. Participant demographics were managed in Excel (Microsoft Corp, Redmond, WA, USA). Thematic analysis followed Colaizzi’s phenomenological approach, a widely established method for deriving meaningful themes from qualitative data to illuminate participants’ experiences, emotions, and behaviours (26). The process included: (i) immersion in the data, (ii) identification of significant statements, (iii) coding and grouping of meanings, (iv) development and refinement of themes, and (v) validation of findings through reflection and comparison with existing literature to ensure interpretive rigour.
RESULTS
General characteristics of study participants
A total of 499 participants completed the survey. The mean age was 68.25 years (SD = 10.44). Among the participants, 298 (59.7%) were male and 372 (74.5%) had ischaemic stroke. The mean time since stroke onset was 12.13 months (SD = 16.33). The modified Rankin Scale (mRS) scores were distributed as follows: 7.0% scored 1, 32.3% scored 2, 42.7% scored 3, and 18.0% scored 4. Detailed characteristics are presented in Table I.
Potential profile analysis of social participation in stroke survivors
Starting with a one-profile model, we incrementally increased the number of profiles using the 3 USER-P subscale scores as indicators. The fit indices for competing models are presented in Table II. When the potential profiles of social participation were 5, the LMR value had no statistical significance (p = 0.497). When the potential profiles of social participation were 4, the entropy value was 0.866, and both the LMR value and the BLRT value were statistically significant (p≤0.05). The AIC, BIC, and aBIC values were all smaller than those when the potential profiles were 2 or 3. Finally, the model with 4 latent profiles was determined to be the best fitting.
A graphical representation of the 4 profiles, based on mean scores of the 3e social participation dimensions, is shown in Fig. 1. The x-axis represents the social participation dimensions, and the y-axis represents the mean scores. Detailed scores and results of pairwise comparisons among profiles are provided in Table III. Each latent profile was named based on its distinctive pattern of scores across the 3 participation dimensions. Profile 1 was termed “Active Integration” (n = 51, 10.2%), characterized by the highest scores in participation frequency, the lowest restrictions, and relatively high satisfaction. Profile 2 was labelled “Contented Conservatism” (n = 67, 13.4%), exhibiting lower participation frequency, moderate restrictions, and high satisfaction levels. Profile 3, named “Cautious Conservatism” (n = 215, 43.1%), showed low frequency, moderate restrictions, and lower satisfaction. Profile 4 was identified as “Alienated Disengagement” (n = 166, 33.3%), with the lowest scores across all 3 dimensions: frequency, restriction, and satisfaction.
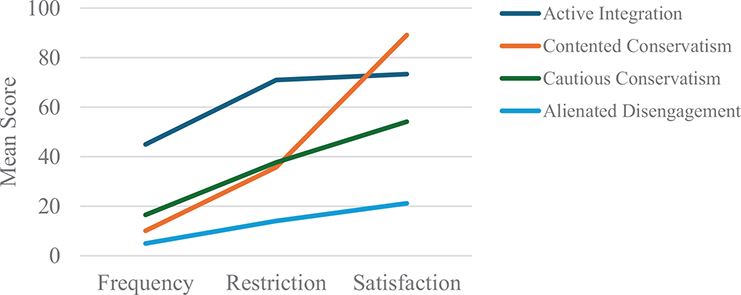
Fig. 1. Characteristics of social participation across four profiles in stroke patients with limb dysfunction.
Multivariate logistic analysis of factors influencing social participation profiles
Univariate analyses were conducted to examine differences in sociodemographic and clinical factors across the 4 profiles (Table IV). Variables that were statistically significant (p < 0.05) in univariate analyses were included as independent variables in a multinomial logistic regression model, with profile membership as the dependent variable. The results of the multivariate logistic regression are presented in Table V. Compared with the “Cautious Conservatism” group, participants with higher resilience and younger age were more likely to belong to the “Active Integration” group; older age, longer disease duration, and female sex were associated with higher likelihood of classification into the “Contented Conservatism” group; lower resilience, poorer physical function, and older age increased the probability of belonging to the “Alienated Disengagement” group.
Qualitative findings
A total of 16 participants were interviewed, reaching data saturation. The sample consisted of 12 males and 4 females, with a mean age of 64.38 years (SD = 12.40). General characteristics of the participants are presented in Table VI. Qualitative analysis identified 5 overarching themes related to behavioural patterns and experiences of social participation among stroke patients.
Behavioural patterns in patients’ social participation
Three primary behavioural patterns emerged from the data regarding how patients approached social participation.
The activist faction referred to the behavioural strategy of stroke patients with limb dysfunction who, under the influence of various factors, actively sought social participation and faced life’s challenges with a positive attitude. They usually took the initiative to engage in social activities, strived to overcome physical barriers, and worked to integrate into society. As 1 participant described it:
Not long after I got sick and came home, I went downstairs by myself. I live on the 4th floor. [Researcher: Was someone accompanying you?] No, who would accompany me? People were afraid to accompany me, worried that if something happened to me, I would sue them for compensation. I relied on myself. Once I could walk around the house by myself, I tried going downstairs. Sometimes, when people kindly saw me and offered to carry things for me, I usually refused. I just relied on myself. If I could move by myself, I would do it on my own.
These participants generally possessed higher levels of resilience, enabling them to adapt more quickly to the challenges brought about by illness. They were not overwhelmed by setbacks and difficulties but were able to adjust their mindset swiftly and face life’s challenges with a positive attitude. Additionally, they tended to be stronger in personality traits and more optimistic in their outlook. They were inclined to rely on their own strength to solve problems. Moreover, this group often benefited from more robust family and social support systems, gaining favourable economic and emotional support as well as abundant social resources and opportunities.
Conservatives were stroke patients with limb dysfunction who, under the influence of various factors, tended to adopt a more cautious and risk-averse behavioural strategy. They usually tried to minimize going out and social activities to avoid potential physical discomfort or accidental risks. These patients often included the ability to participate in social activities, but expressed significant psychological concerns. As P4 explained:
I don’t really dare to go out. Previously, we used to walk by the river every day, greeting each other. Later, she didn’t show up for three days, and they said she had passed away and was already cremated. So, I don’t really dare to go out now and just stay active in the neighbourhood.
This patient, having experienced the sudden death of a companion, became more concerned about her health and preferred to limit her social activities to the immediate community. The spouse of P8 added:
He once walked too fast and fell, knocking out a tooth. He was terrified. So now he walks very slowly, one step at a time, as if he’s stepping on ants [P8: It’s okay to walk slowly], very slowly, like the way elderly people walk.
Another spouse noted: “He has fallen three times before, but fortunately, he didn’t fracture any bones. So now we are very careful and don’t let him go out alone” (P1’s spouse).
Stroke patients with limb dysfunction frequently experienced poor balance, weak muscle strength, and instability, which increased the risk of falling. Many stroke patients, especially those with prior fall experiences, became more conservative in their social activities, prioritizing safety while maintaining their physical functions. Patients with this behavioural strategy was influenced not only by their physical func-tions but also by other factors, such as negative past experiences in social participation, lack of confidence in their ability to engage socially, overprotection from family members, and unfavourable environmental conditions.
The alienated group comprised stroke patients with physical disabilities who, due to a multitude of factors, experienced a decrease in motivation and willingness to participate socially, maintaining a low-intensity, static level of engagement. “Since getting sick, I haven’t used my mobile phone or computer, cutting off my connection with the outside world” (P2). The alienated group was closely related to the impaired physical functions. The physical limitations such as inconvenience in movement and restricted activity capabilities made patients experience a sense of loss of control and feel incapable when facing social participation, thus reducing their motivation and willingness to engage. Additionally, changes in body image may impacted their self-esteem, thereby reducing their willingness to engage in social activities and leading them to actively sever social interactions. This pattern also correlated with lower resilience levels; these patients often lacked sufficient adaptive capacity to actively cope with life’s changes and challenges, thus causing them to prefer an avoidant way of living. Furthermore, it may also be related to inadequate family and social support, as well as unfavourable environmental conditions.
Emotional experience of patients’ social participation
Sense of loss described the complex emotional experience of stroke patients with physical disabilities, who, when reviewing and comparing their social participation before and after the onset of the disease, subjectively perceived a significant decrease in their ability or opportunity to fulfil roles, engage in activities, connect with others, and achieve self-worth across multiple dimensions. This led to a profound and persistent feeling of longing and loss. The essence of the sense of loss was that these patients habitually compared their current state with the period before the stroke. Therefore, when asked about their views on current social participation, these patients often expressed that “It’s incomparable to before the illness; I can’t do XX anymore” (for example, P3 described I thus: “This condition greatly affects life, there’s no way around it, now I can’t even travel”). While decreased social participation following stroke represented an objective reality for most patients with physical disabilities, continuously making such comparisons intensified their sorrowful feelings and hindered current social engagement. As P8’s spouse recounted, “He has nothing much to do, just sits on the sofa, and when I ask if he wants to go out, he gets very irritable and says, ‘I’m not in the mood today, I don’t want to go out’”.
The sense of loss appeared closely related to the rigid self-identity of stroke patients with physical disabilities and the absence of downward comparison. In psychology, self-identity refers to an individual’s understanding and perception of who they are, and what traits, values, and goals they possess (27). It is an important part of self-awareness and reflects a person’s internal perception of their identity (28). When stroke patients with physical disabilities tightly bound their self-concept to the “intact” state before the illness, it became relatively more difficult to integrate the “disabled” state after the illness into a new, equally valuable self-identity. These patients demonstrated limited identification and trust in their “disabled” self, and thus showed a lack of interest in social participation across multiple dimensions such as role fulfilment, activity range, interpersonal connections, and self-worth achievement. As P1’s spouse said, “He seems to have lost interest in these activities”. The second possible reason for the sense of loss involved the absence of downward comparison. Downward social comparison is an important concept in social comparison theory, first proposed by psychologist Leon Festinger in 1954 (29). It refers to individuals comparing themselves with those who are doing worse, thereby enhancing their self-esteem and self-evaluation. When stroke patients with physical disabilities engaged in effective downward comparison, such as recognizing their own survival and considering others in worse conditions, it helped alleviate negative emotions and strengthen confidence in dealing with setbacks. As P11 described it, “I went to the rehabilitation hospital for recovery, and there were many people in worse conditions than me.” However, when patients lacked downward comparison, they were more likely to remain stuck in a rigid self-identity, leading to a more severe sense of loss in social participation.
The sense of rebuilding captured the positive psychological experience of stroke patients with physical disabilities, who, after experiencing the significant impact of the disease, through continuous efforts, adaptation, and adjustment, compared their current social participation with the state immediately after the onset of the disease. They subjectively perceived a significant improvement in their ability or opportunity to fulfil roles, engage in activities, connect with others, and achieve self-worth across multiple dimensions. The essence of the sense of rebuilding involved comparing the current social participation with the period of most severe functional impairment (usually immediately after the onset or the acute phase). Therefore, when asked about their views on current social participation, patients often expressed that “It’s much better than when I first got sick”; such as when P13 said:
At first, the doctor told me that I might have to lie in bed for the rest of my life, but now I have recovered well enough to walk, although I’m not stable and have poor balance, but I have recovered quite well. Last year, I was even cooking, but this year, because the stove was slippery, I can’t cook with one hand.
Although this sense of rebuilding does not necessarily require the patient’s physical function to recover to a normal level, and the patient may still have irreversible physical function damage and lifelong disability, comparing with the worst state after the disease onset helped the patient face current social life with a positive attitude. “When I first got out of the hospital, I couldn’t do anything, but now I can walk with a limp and even cook for myself, one meat dish and one vegetable dish, taking care of my spouse, all by myself” (P7).
The possible reason for the sense of rebuilding was the patient’s acceptance of the disease. After experiencing a significant event, patients who accepted reality acknowledged disability as their new reality and discovered new meaning and possibilities based on this acceptance. These patients were more inclined to focus on the present, shifting their goals from “returning to the past” to “achieving the best functional state”. They were more likely to take proactive approaches to explore social activities they can participate in with their current abilities.
Researcher: You just described facing many difficulties when going downstairs. Can you describe how you feel about it? “It’s all about mindset, it depends on yourself, that’s enough. Without a strong will, what do you have? What’s the point of living? You have to have flavour, life has to have flavour, that’s it.” (P7)
Despite having physical disabilities (mRS score of 2) and needing to care for a spouse with a mental disorder who is bedridden, this research subject did not complain about his current situation during the 72-min interview. His use of the word “flavour,” full of warmth, to describe his life, demonstrated both his acceptance of the stroke and his efforts to return to society in his own way.
The sense of loss and the sense of rebuilding are best understood not as a binary dichotomy, but as anchoring a spectrum of emotional experiences of social participation. They could coexist in the same individual in varying degrees and change with different stages of the disease process. The sense of loss constituted a natural reaction to the catastrophic event of stroke, but when it persisted and solidified, it became a major obstacle to social participation. In contrast, the sense of rebuilding reflected the patient’s resilience and adaptability, representing a positive subjective experience of social participation.
Quantitative–qualitative integration
The integration of quantitative and qualitative findings is summarized in Fig. 2. Quantitatively, the “Active Integration” profile was characterized by high participation frequency, low restrictions, and high satisfaction, which aligned cohesively with the qualitative activist faction behavioural pattern and was predominantly guided by a sense of rebuilding. The qualitative analysis defined the sense of rebuilding as an emotional experience characterized by acceptance of reality, and a positive mindset – an internal state logically associated with higher social participation satisfaction. A particularly revealing contrast emerged between the “Contented Conservatism” and “Cautious Conservatism” profiles. While both exhibited similar moderate participation frequency and restrictions and corresponded to the conservatives behavioural pattern, they diverged fundamentally in their emotional drivers and resulting satisfaction. The high satisfaction in the “Contented Conservatism” profile was interpreted as being underpinned by a sense of rebuilding, explaining how individuals achieved contentment within a limited scope of activities. In contrast, the lower satisfaction in the “Cautious Conservatism” profile was linked to a sense of loss (characterized by grief over functional decline and a focus on the pre-stroke self), which is logically associated with diminished satisfaction. The “Alienated Disengagement” profile, defined by very low frequency, very high restrictions, and very low satisfaction, formed a coherent cluster with the qualitative alienated group behavioural pattern and a dominant sense of loss. In fact, the emotional experiences of stroke patients are distributed along a continuum between a sense of rebuilding and a sense of loss. Although Fig. 2 only marks these 2 endpoints on the horizontal axis, we conceptualize patients’ emotional positioning across this spectrum. Specifically, individuals with higher satisfaction scores (Active Integration and Contented Conservatism) are positioned closer to the sense of rebuilding, while those with lower satisfaction (Cautious Conservatism and Alienated Disengagement) are located nearer to the sense of loss.

Fig. 2. Quantitative–qualitative integration.
DISCUSSION
This study identified 4 distinctive profiles of social participation of stroke survivors with limb dysfunction through LPA (Active Integration, Contented Conservatism, Cautious Conservatism, and Alienated Disengagement), and through qualitative research we deeply depicted the unique behavioural patterns (activist faction, conservatives, and alienated group) and dominant emotional experiences (sense of rebuilding and sense of loss) of each profile. This study was one of the first to assess in depth the heterogeneity and internal experiences of social participation of this group within the Chinese cultural context using a mixed-method approach. The integration of quantitative and qualitative results provides a more comprehensive and multi-faceted perspective for understanding the complexity of social participation.
Our findings indicate that 10.2% of survivors, categorized as “Active Integration”, maintain a relatively high frequency of social participation and report positive participatory experiences. Qualitative data reveal that these individuals tend to engage proactively in social activities and perceive their current involvement more favourably by comparing it with their condition shortly after diagnosis. Notably, another 13.4% of participants, classified as “Contented Conservatism”, report high satisfaction with social participation despite experiencing noticeable restrictions. Qualitative insights suggest that this contentment stems largely from a feeling of “rebuilding”, consistent with previous studies indicating that the quality (rather than the frequency or quantity) of social participation is central to subjective experience (30). These results carry important clinical implications: for this subgroup of stroke survivors, interventions should emphasize enhancing the meaning and quality of social engagement rather than merely increasing the number of activities. Rather than striving to expand the range of participative acts, support efforts should focus on helping individuals accept the irreversible aspects of their disability and identify forms of participation that align with their current needs and values (31). This person-centred, quality-oriented approach represents a shift beyond conventional intervention strategies that have traditionally prioritized quantitative increases in social activity.
Furthermore, this study revealed that 43.1% of stroke survivors (Cautious Conservatism) exhibited moderate levels of social participation restriction, frequency, and satisfaction. In contrast, 33.3% of survivors (Alienated Disengagement) showed high levels of restriction alongside low frequency and satisfaction. These results indicate that the majority of stroke survivors with physical disabilities experience relatively limited social participation and report unsatisfactory participatory experiences (32). Importantly, impaired social participation cannot be attributed solely to physical dysfunction; it is also closely associated with participants’ engagement strategies and psychological attitudes. Consequently, clinical interventions should not only focus on physical function training, such as virtual reality (33), robotic technology (34), and other rehabilitation devices (35, 36), but must also prioritize psychological adjustment. Enhancing motivation, fostering a positive attitude toward social reintegration, and supporting survivors in actively engaging with post-disability social life are critical components of effective rehabilitation (37, 38). It is particularly noteworthy that while quantitative measures of participation behaviour were similar between the “Contented Conservatism” and “Cautious Conservatism” groups, their levels of satisfaction differed significantly. Qualitative results identified that a sense of rebuilding vs a sense of loss served as the key differentiator influencing satisfaction. The sense of rebuilding reflects the patients’ acceptance of their disease and disability, which can serve as a powerful psychological resource (39, 40), enabling individuals to adopt a constructive attitude towards social life, for example by actively seeking help, thereby expanding opportunities and conditions for participation. The 4-profile classification also suggests that improving social participation does not necessarily require all patients to achieve the highest engagement level. Instead, a progressive, profile-based approach is recommended, for instance, supporting transition from Alienated Disengagement to Cautious Conservatism, or from Contented Conservatism to Active Integration. These findings provide a valuable evidence base for developing targeted clinical interventions tailored to patients’ specific social participation patterns.
This study revealed that individuals with higher levels of resilience were more likely to belong to the “Active Integration” profile, whereas those with lower resilience tended to be classified as “Alienated Disengagement”. However, resilience levels did not significantly influence classification into the “Contented Conservatism” or “Cautious Conservatism” profiles. These findings align with previous research supporting a positive correlation between resilience and social participation (41). Resilience is conceptualized as a dynamic process of positive adaptation in the face of adversity or trauma (42). Previous studies indicate that individuals with greater resilience are better equipped to mobilize internal and external resources, facilitating rapid recovery from negative experiences and buffering the impact of stressors (43). Recent evidence further suggests that resilience facilitates neuroplasticity and adaptive processes through the distinct yet synergistic actions of catecholamines (such as dopamine and norepinephrine) and glucocorticoids (44). In the context of stroke recovery, survivors with higher resilience demonstrate an enhanced capacity to adapt to disability-related changes and challenges. These individuals demonstrate a proactive approach and achieve higher levels of social engagement. Crucially, they also derive genuine satisfaction from their social experiences. Therefore, resilience should be considered a key target for interventions aimed at improving social participation in stroke patients with physical disabilities.
The study also found that, compared with the Cautious Conservatism profile, individuals with poorer limb function were more likely to be classified into the Alienated Disengagement profile, while limb function did not significantly influence classification into the remaining categories. This finding both aligns with and interestingly extends a substantial body of prior research emphasizing that “physical function is a key determinant of social participation” (45, 46). First, significant deterioration in limb function may act as the “final straw” that overwhelms a patient’s willingness to participate socially, pushing them into a state of Alienated Disengagement. When functional impairment reaches a certain severity (e.g., mRS grade 4), it creates an almost insurmountable objective barrier, rendering most social activities physically “impossible” or “extremely difficult”, thereby directly causing a sharp decline in both participation frequency and satisfaction. This aligns with the classical paradigm established in previous studies. However, more importantly, limb function did not significantly distinguish among the Active Integration, Contented Conservatism, and Cautious Conservatism profiles. This suggests that physical capacity is not the dominant differentiating factor in social participation patterns until a certain threshold of severe disability is reached. Instead, psychological and emotional factors likely play a more central role than objective physical function. Therefore, the findings of this study refine the traditional linear understanding that better function leads to better participation and propose a more nuanced model: Limb function is a prerequisite for social participation, but it alone is not sufficient to determine its nature or quality. It plays a decisive role when impairment is severe (defining the lower bound of participation), but within the range of moderate dysfunction, individual psychological and cognitive factors (47), such as resilience, comparison strategies, and self-identity, serve as the critical watershed that determines whether one ultimately follows an Active, Contented, or Cautious path.
Furthermore, this study identified age as a significant factor differentiating social participation profiles. Younger age predicted membership in the Active Integration profile, whereas older age increased the likelihood of Contented Conservatism or Alienated Disengagement, consistent with existing literature (48). Physiologically, the greater resilience and neuroplasticity of younger patients support faster recovery, enabling active reintegration. In contrast, older adults often face comorbidities and functional decline, predisposing them to disengagement (49). Social roles also contribute: younger individuals are often driven by familial or occupational duties, while older adults, frequently retired, may either adapt contentedly to reduced roles or experience significant loss (50). Rehabilitation strategies should thus be age-specific: supporting younger patients in reclaiming social roles, and assisting older adults in constructing new, meaningful forms of participation. Additionally, this study found that females were more likely to belong to the Contented Conservatism profile than to Cautious Conservatism, which contrasts with previous reports of no significant gender differences in participation satisfaction (51). This discrepancy may reflect traditional gender roles in Chinese society, where women are often socialized to prioritize family harmony. Such expectations may encourage emotion regulation, cognitive reframing, and downward comparison, enabling them to find satisfaction in manageable activities like household tasks.
Limitations
Several limitations should be acknowledged. First, the cross-sectional design precludes establishing causal relationships between the identified predictors and profile membership. Longitudinal studies are needed to examine the stability of these profiles and their trajectories over time. Second, the generalizability of the findings may be limited as participants were recruited solely from rehabilitation centres in Shanghai, and the qualitative sample exhibited a gender imbalance (with more males), which may not fully represent potential gender-specific experiences. Future multi-centre studies with more diverse sampling are warranted. Third, the exclusion of patients with cognitive impairments and communicative disorders may limit the generalizability of our findings to the broader stroke population. Fourth, although a mixed-methods approach was employed, the potential for common method bias in the self-reported quantitative data remains. Finally, environmental factors, such as community accessibility and social policies, were not quantitatively assessed and integrated into the predictive model, representing an important avenue for future research. Specifically, future studies could quantitatively investigate the impact of specific policies (e.g., long-term care insurance) and built environment factors on social participation profiles, employing longitudinal or multi-centre designs.
Conclusion
This study employed a convergent mixed-methods design to systematically reveal, for the first time, 4 heterogeneous latent profiles of social participation among Chinese stroke patients with limb dysfunction: “Active Integration”, “Contented Conservatism”, “Cautious Conservatism”, and “Alienated Disengagement”. Each profile is distinguished not only by objective manifestations of social participation (frequency, restrictions) but also by unique primary behavioural patterns (active, conservative, alienated) and dominant emotional experiences (sense of rebuilding, sense of loss). Clinical practitioners should acknowledge this heterogeneity and adopt a precision strategy of “tailored intervention based on profiling” and “step-by-step enhancement” to effectively improve patients’ overall level of social participation and quality of life.
ACKNOWLEDGEMENTS
Availability of data and materials: Data supporting this research are available upon reasonable request. Please contact the corresponding author for access.
REFERENCES
- Feigin VL, Brainin M, Norrving B, Martins SO, Pandian J, Lindsay P, et al. World Stroke Organization: Global stroke fact sheet 2025. Int J Stroke 2025; 20: 132–144. https://doi.org/10.1177/17474930241308142
- Tu WJ, Wang LD; Special Writing Group of China Stroke Surveillance Report. China stroke surveillance report 2021. Mil Med Res 2023; 10: 33. https://doi.org/10.1186/s40779-023-00463-x
- Kumar S, Chou SH, Smith CJ, Nallaparaju A, Laurido-Soto OJ, Leonard AD, et al. Addressing systemic complications of acute stroke: a scientific statement from the American Heart Association. Stroke 2025; 56: e15–e29. https://doi.org/10.1161/STR.0000000000000477
- Woodman P, Riazi A, Pereira C, Jones F. Social participation post stroke: a meta-ethnographic review of the experiences and views of community-dwelling stroke survivors. Disabil Rehabil 2014; 36: 2031–2043. https://doi.org/10.3109/09638288.2014.887796
- Norlander A, Iwarsson S, Jönsson A, Lindgren A, Lexell E. Participation in social and leisure activities while re-constructing the self: understanding strategies used by stroke survivors from a long-term perspective. Disabil Rehabil 2022; 44: 4284–4292. https://doi.org/10.1080/09638288.2021.1900418
- Yan J, Wang Y, Zhang L, Chen P, Yang N, Zhang H. Social participation of stroke patients: a bibliometric analysis. Front Neurol 2025; 16: 1616861. https://doi.org/10.3389/fneur.2025.1616861
- de Souza F, Sales M, Laporte L, Melo A, da Silva Ribeiro N. Discharge outcomes as predictors of social participation in the community after a stroke: a cohort study. Int J Rehabil Res 2023; 46: 325–330. https://doi.org/10.1097/MRR.0000000000000599
- Wan X, Chan DNS, Chau JPC, Zhang Y, Gu Z, Xu L. Social participation challenges and facilitators among Chinese stroke survivors: a qualitative descriptive study. BMC Public Health 2025; 25: 468. https://doi.org/10.1186/s12889-025-21592-z
- Vecchia CD, Préau M, Haesebaert J, Viprey M, Rode G, Termoz A, et al. Factors associated with post-stroke social participation: a quantitative study based on the ICF framework. Ann Phys Rehabil Med 2023; 66: 101686. https://doi.org/10.1016/j.rehab.2022.101686
- Gingrich N, Bosancich J, Schmidt J, Sakakibara BM. Capability, opportunity, motivation, and social participation after stroke. Top Stroke Rehabil 2023; 30: 423–435. https://doi.org/10.1080/10749357.2022.2070358
- Foley EL, Nicholas ML, Baum CM, Connor LT. Influence of environmental factors on social participation post-stroke. Behav Neurol 2019; 2019: 2606039. https://doi.org/10.1155/2019/2606039
- Zhou X, Du M, Dai X, Zhu S, Zhou L, Li X. Intervention patterns and preliminary effectiveness on social participation following stroke: a scoping review. BMC Neurol 2023; 23: 275. https://doi.org/10.1186/s12883-023-03250-2
- Zhang Q, Schwade M, Smith Y, Wood R, Young L. Exercise-based interventions for post-stroke social participation: a systematic review and network meta-analysis. Int J Nurs Stud 2020; 111: 103738. https://doi.org/10.1016/j.ijnurstu.2020.103738
- Qiao X, Wu Z, Ren Y, Li Y. Effectiveness of the Dyadic Coping Intervention of Social Participation (DCISP) for stroke survivors: study protocol for a randomized controlled trial. BMC Psychol 2024; 12: 500. https://doi.org/10.1186/s40359-024-01994-1
- Xue M, Wang Q, Wang J, Ge S, Zhang Z, Mei Y. E-health literacy in stroke patients: latent profile analysis and influencing factors. J Adv Nurs 2025; 81: 1388–1398. https://doi.org/10.1111/jan.16351
- Lin S, Wang C, Wang Q, Xie S, Tu Q, Zhang H, et al. The experience of stroke survivors and caregivers during hospital-to-home transitional care: a qualitative longitudinal study. Int J Nurs Stud 2022; 130: 104213. https://doi.org/10.1016/j.ijnurstu.2022.104213
- Tovin MM, Wormley ME. Systematic development of standards for mixed methods reporting in rehabilitation health sciences research. Phys Ther 2023; 103: pzad084.
- Ferguson SL, EWG Moore, DM Hull. Finding latent groups in observed data: a primer on latent profile analysis in Mplus for applied researchers. Int J Behav Dev 2020; 44: 458–468. https://doi.org/10.1093/ptj/pzad084
- van der Zee CH, Priesterbach AR, van der Dussen L, Kap A, Schepers VPM, Visser-Meily JMA, et al. Reproducibility of three self-report participation measures: the ICF Measure of Participation and Activities Screener, the Participation Scale, and the Utrecht Scale for Evaluation of Rehabilitation-Participation. J Rehabil Med 2010; 42: 752–757. https://doi.org/10.2340/16501977-0589
- de Graaf JA, Volkers EJ, Schepers VPM, Visser-Meily JMA, Post MWM. Validity of the Utrecht scale for evaluation of rehabilitation-participation restrictions scale in a hospital based stroke population 3 months after stroke. Top Stroke Rehabil 2022; 29: 516–525. https://doi.org/10.1080/10749357.2021.1956047
- Zhang ZY. The translation and validation of the Utrecht Scale for Evaluation of Rehabilitation-Participation (USER-P) in a Chinese context. Master’s thesis, Soochow University; 2016.
- Yu X, Zhang J. Factor analysis and psychometric evaluation of the Connor-Davidson resilience scale (CD-RISC) with Chinese people. Soc Behav Pers 2007; 35: 19–30. https://doi.org/10.1186/s12888-017-1219-0
- Yu XN, Lau JT, Mak WW, Zhang J, Lui WWS, Zhang J. Factor structure and psychometric properties of the Connor Davidson Resilience Scale among Chinese adolescents. Compr Psychiatry 2011; 52: 218–224. https://doi.org/10.1016/j.comppsych.2010.05.010
- Wu Z, Liu Y, Li X, Li X. Resilience and associated factors among mainland Chinese women newly diagnosed with breast cancer. PLoS One 2016; 11: e0167976. https://doi.org/10.1371/journal.pone.0167976
- Fan Yuhua, Ji Xiaoyun, Lan Linfang. Application of the modified Rankin Scale in efficacy assessment of domestic stroke clinical trials. Chin J Nerv Ment Dis 2015; 7: 412–415. https://doi.org/10.3969/j.issn.1002-0152.2015.07.006
- Colaizzi PF. Psychological research as the phenomenologist views it. In: Valle RS, King M, editors. Existential-phenomenological alternatives for psychology. New York: Oxford University Press; 1978, p. 48–71.
- Wheeler SC, Bechler CJ. Objects and self-identity. Curr Opin Psychol 2021; 39: 6–11. https://doi.org/10.1016/j.copsyc.2020.07.013
- Gu T, Cheng Z, Zhang Z, Li C, Ni Y, Wang X. Formation mechanism of contributors’ self-identity based on social identity in online knowledge communities. Front Psychol 2022; 13: 1046525. https://doi.org/10.3389/fpsyg.2022.1046525
- Gerber JP, Wheeler L, Suls J. A social comparison theory meta-analysis 60+ years on. Psychol Bull 2018; 144: 177–197. https://doi.org/10.1037/bul0000127
- Zhou X, Du M, Weng Y, Zhou L. Hard return: the development and transformation process of social participation in stroke survivors; a qualitative study and initial theory. Clin Rehabil 2020; 34: 824–836. https://doi.org/10.1177/0269215520917191
- Ozkan H, Ambler G, Banerjee G, Mitchell JJ, Barbato C, Browning S, et al. Prevalence, predictors, and patterns of patient reported non-motor outcomes six months after stroke: a prospective cohort study. Lancet Reg Health Eur 2024; 47: 101080. https://doi.org/10.1016/j.lanepe.2024.101080
- Bailliard AL, Singsomphone L, Kim N, Li SY, Vutakuri N, Ougui H, et al. Life after stroke: changes in sensory health and the impact on participation. Top Stroke Rehabil 2025; 32: 586–594. https://doi.org/10.1080/10749357.2024.2435659
- Krohn M, Rintala A, Immonen J, Sjögren T. The effectiveness of therapeutic exercise interventions with virtual reality on balance and walking among persons with chronic stroke: systematic review, meta-analysis, and meta-regression of randomized controlled trials. J Med Internet Res 2024; 26: e59136. https://doi.org/10.2196/59136
- Yildiz A, Ahmed I, Mustafaoglu R, Kesiktas FN. Effects of robot-assisted arm training on respiratory muscle strength, activities of daily living, and quality of life in patients with stroke: a single-blinded randomized controlled trial. Physiother Theory Pract 2024; 40: 2818–2826. https://doi.org/10.1080/09593985.2023.2299727
- Fluet G, Qiu Q, Gross A, Gorin H, Patel J, Merians A. The influence of scaffolding on intrinsic motivation and autonomous adherence to a game-based, sparsely supervised home rehabilitation program for people with upper extremity hemiparesis due to stroke: a randomized controlled trial. Journal of Neuroengineering and Rehabilitation 2024; 21: 143. https://doi.org/10.1186/s12984-024-01441-7
- Chang CS, Chen CL, Chen RS, Chen HC, Chen CY, Chung CY, et al. Synergistic efficacy of repetitive peripheral magnetic stimulation on central intermittent theta burst stimulation for upper limb function in patients with stroke: A double-blinded, randomized controlled trial. J Neuroeng Rehabil 2024; 21: 49. https://doi.org/10.1186/s12984-024-01341-w
- Bollinger RM, Krauss MJ, Somerville EK, Holden BM, Blenden G, Hollingsworth H, et al. Rehabilitation transition program to improve community participation among stroke survivors. JAMA Netw Open 2024; 7: e2437758. https://doi.org/10.1001/jamanetworkopen.2024.37758
- Lo SHS, Chau JPC, Lau AYL, Choi KC, Shum EWC, Lee VWY, et al. Virtual multidisciplinary stroke care clinic for community-dwelling stroke survivors: a randomized controlled trial. Stroke 2023; 54: 2482–2490. https://doi.org/10.1161/STROKEAHA.123.043605
- Shi Y, Liang Z, Zhang Y, Zhou Y, Dong S, Li J, et al. Latent profiles of psychological resilience in patients with chronic disease and their association with social support and activities of daily living: Title page. BMC Psychol 2025; 13: 792. https://doi.org/10.1186/s40359-025-03115-y
- Burke A, Davoren MP, Arensman E, Harrington JM. Psychoeducational interventions for people living with chronic communicable disease: a systematic review. BMJ Open 2024; 14: e077007. https://doi.org/10.1136/bmjopen-2023-077007
- Zhou X, Wang Y, Zhou L. Social participation, resilience, and coping tendency in a sample of stroke survivors: a multi-centre cross-sectional study in China. J Rehabil Med 2024; 56: jrm12448. https://doi.org/10.2340/jrm.v56.12448
- American Psychology Association Help Center. The road to resilience: what is resilience? [EB/OL]. 2011 [cited 2017 Jan 6]. Available from: http://www.apa.org/helpcenter/roadresilience.aspx
- Jeste DV, Alexopoulos GS, Blazer DG, Lavretsky H, Sachdev P, Reynolds CF. Wisdom, resilience, and well-being in later life. Annu Rev Clin Psychol 2025; 21: 33–59. https://doi.org/10.1146/annurev-clinpsy-081423-031855
- Hermans EJ, Hendler T, Kalisch R. Building resilience: the stress response as a driving force for neuroplasticity and adaptation. Biol Psychiatry 2025; 97: 330–338. https://doi.org/10.1016/j.biopsych.2024.10.016
- Chang FH, Lin YN, Liou TH, Ni PS. Predicting trends of community participation after hospital discharge for younger adults after stroke. Ann Phys Rehabil Med 2023; 66: 101644. https://doi.org/10.1016/j.rehab.2022.101644
- Liu Y, Li T, Ding L, Cai ZX, Nie S. A predictive model for social participation of middle-aged and older adult stroke survivors: the China Health and Retirement Longitudinal Study. Front Public Health 2024; 11: 1271294. https://doi.org/10.3389/fpubh.2023.1271294
- Li Y, Zhang W, Ye M, Zhou L. Perceived participation and autonomy post-stroke and associated factors: an explorative cross-sectional study. J Adv Nurs 2021; 77: 1293–1303. https://doi.org/10.1111/jan.14670
- Hoyle M, Meredith P, Ownsworth T, Khan A, Gustafsson L. Associations between participation and personal factors in community-dwelling adults post-stroke. Brain Impair 2023; 24: 456–473. https://doi.org/10.1017/BrImp.2022.31
- Markle-Reid M, Fisher K, Walker KM, Beauchamp M, Cameron JI, Dayler D, et al. The stroke transitional care intervention for older adults with stroke and multimorbidity: a multisite pragmatic randomized controlled trial. BMC Geriatr 2023; 23: 687. https://doi.org/10.1186/s12877-023-04403-1
- Zhang H, Sun S, Ma L, Abudureyimu A, Xiu M, Li K, et al. “Flexible trade-off”: social participation change model among middle-aged and older stroke survivors: a grounded theory study. J Gerontol B Psychol Sci Soc Sci 2025; 80: gbaf09. https://doi.org/10.1093/geronb/gbaf091
- de Graaf JA, van Miltenburg S, Wermer MJH, Post MWM, Visser-Meily JMA. Gender differences in participation one year after stroke: exploring biopsychosocial predictors for women and men. Top Stroke Rehabil 2025; 32: 150–160. https://doi.org/10.1080/10749357.2024.2377518