REVIEW ARTICLE
ROBOT-ASSISTED THERAPY FOLLOWING STROKE: WHAT EFFECTS ON QUALITY OF LIFE, COGNITIVE AND PSYCHOSOCIAL OUTCOMES? A SYSTEMATIC REVIEW
Francesco ZANATTA, PhD1  , Alessandra GORINI, PhD2,3 , Luca FIORENTINO, MsC2, Silvia TRAVERSONI, MsC2 , Cira FUNDARÒ, MD4 , Marco D’ADDARIO, PhD1 and Patrizia STECA, PhD1
, Alessandra GORINI, PhD2,3 , Luca FIORENTINO, MsC2, Silvia TRAVERSONI, MsC2 , Cira FUNDARÒ, MD4 , Marco D’ADDARIO, PhD1 and Patrizia STECA, PhD1
From the 1Department of Psychology, University of Milano-Bicocca, Milan, 2Department of Clinical Sciences and Community Health, Department of Excellence 2023-2027, University of Milan, Milan, 3PsyCaRe Lab, Istituti Clinici Scientifici Maugeri IRCCS, Milan, and 4Neurophysiopathology Unit, Istituti Clinici Scientifici Maugeri IRCCS, Montescano Institute, Montescano, Italy
Objective: Robot-assisted therapy (RAT) has shown promise in post-stroke motor recovery. However, its effects on non-motor outcomes remain unclear. This systematic review evaluated RAT impact on post-stroke quality of life (QoL), cognition, and psychosocial functioning.
Methods: Following PRISMA guidelines, electronic searches were performed from Web of Science, PubMed, Cochrane Library, CINAHL, Embase, and PsycINFO. Risk of bias was assessed using NIH Quality Assessment Tools. Data on study design, participants, intervention characteristics, outcomes, and results were extracted and synthetized descriptively.
Results: A total of 90 studies met the inclusion criteria. Considerable heterogeneity was found in participants’ characteristics, intervention duration (2–52 weeks), and dosage (20–240 min/session). Most studies reported significant RAT effects on QoL (emotional, physical, cognitive, social subdomains), cognition (attention, executive functions, memory, language, visuo-spatial abilities, intelligence), and psychosocial outcomes (anxiety, depression, self-efficacy, fear of falling, motivation, coping). Some studies also showed greater improvements compared with conventional training controls. Longitudinal effects were generally absent, except for QoL variations observed up to 12 months. Cognitive and psychological factors were also identified as moderators/predictors of RAT response.
Conclusion: Despite variability across studies, findings suggest RAT may have a broad impact beyond motor recovery. Future large-scale, standardized, longitudinal trials are recommended to confirm these results.
LAY ABSTRACT
After a stroke, many people struggle not only with movement but also with thinking, emotions, and social life. Robot-assisted therapy is a new rehabilitation approach that helps patients perform repeated and precise movements with robotic support. We reviewed the studies of the last 2 decades to understand whether this therapy also improves aspects of life beyond movement. The results show that robot-assisted therapy can have positive effects on quality of life, mood, memory, attention, and well-being. Some studies even found better outcomes than with traditional rehabilitation. However, the improvements did not always last over time, and the studies differed in duration and intensity. Overall, our findings suggest that robot-assisted therapy could support more complete recovery after stroke, addressing both body and mind. Further research is still needed to confirm its long-term benefits for everyday clinical practice.
Key words: stroke; rehabilitation; robot-assisted therapy; systematic review; cognition; quality of life.
Citation: J Rehabil Med 2026; 58: jrm44943. DOI: https://doi.org/10.2340/jrm.v58.44943.
Copyright: © 2026 The Author(s). Published by MJS Publishing, on behalf of the Foundation for Rehabilitation Information. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/).
Submitted: Oct 22, 2025; Accepted after revision: Jan 9, 2026; Published: Feb 11, 2026.
Correspondence address: Alessandra Gorini, Department of Clinical Sciences and Community Health, University of Milan, Milan, Italy. E-mail: alessandra.gorini@unimi.it
Competing interests and funding: The authors have no conflicts of interest to declare.
The project is funded by the Italian Ministry of University and Research (MUR) under the Scheme Research Projects of National Interest (PRIN prot. N. 20227BY8BA).
Over the past decades, population ageing has been increasing worldwide, contributing to a progressive rise in the incidence of various complex and chronic diseases, including stroke. According to the most recent global estimates, stroke accounted for approximately 93.8 million (89–99.3) cases and 7.3 million (6.6–7.8) deaths. Its impact, however, extends far beyond mortality and has presented significant challenges related to disability and quality of life (QoL) by accounting for a total of 160 million (148–172) Disability-Adjusted Life Years (DALYs) worldwide and an increase of 32.2% (21.7–42.6) over the last 20 years (1). Such global trends, along with the projected increase in stroke survivors, not only underscore the growing demand for long-term care and efficient rehabilitation services, but also focus attention on the necessity of addressing patients’ global functioning, as conceptualized within a biopsychosocial framework encompassing body structures and functions, activities, and participation in everyday life (2). Accordingly, given the multifaceted consequences of stroke, comprehensive, impactful, and sustained strategies are increasingly required.
Over the last years, the field of neurorehabilitation has increasingly embraced technology innovation to improve recovery outcomes (3). A prominent approach is robot-assisted therapy (RAT), which has gained considerable attention for its ability to enable highly tailored rehabilitation protocols along with repetitive, intensive, and task-oriented exercises that align with the principles of motor relearning and neuroplasticity (4, 5). RAT devices, including exoskeletons, end-effector systems, and soft-robots have so far provided customizable and controlled training paradigms that have efficiently supported the recovery of both upper and lower limb functions (6). Exoskeletons are wearable robotic systems composed of mechanical and electronic components that fully or partially align with a patient’s limb segment, guiding and assisting movement according to predefined kinematic or dynamic trajectories. End-effector devices, in contrast, interface only with the distal part of the limb, allowing movement to emerge more freely through the activation of a patient’s residual motor control, with fewer biomechanical constraints and a greater number of degrees of freedom. Soft-robots represent a more recent category of lightweight and flexible wearable devices, originally developed to support activities of daily living (ADLs) but increasingly applied in rehabilitation due to their adaptability and comfort. Compared with conventional motor training, these robotic approaches allow greater training intensity, precise control of movement parameters, and enriched task-oriented feedback. More recently, a growing body of research suggested that RAT can extend its potential beyond motor recovery, too. The repetitive and goal-directed nature of RAT, often combined with augmented visual or sensory feedback, may stimulate cognitive domains such as attention, executive functions, and learning processes through shared neural networks underlying motor and cognitive control. Moreover, increased patient engagement, motivation, and perceived self-efficacy during enhanced training may positively influence psychological outcomes. These advancements are particularly evident in the context of stroke rehabilitation, where RAT has shown promise to address a wider spectrum of patient symptoms, including cognitive deficits, functional impairment, and reduced psychosocial well-being (7–9).
Patients recovering from stroke often exhibit heterogeneous functional profiles, with cognitive impairments across various domains significantly impacting overall recovery. Commonly affected areas include attention, executive function, memory, language and visuo-spatial abilities, although the evidence on the domain-specific cognitive effects of rehabilitation remains limited (10, 11). Additionally, mental health issues are prevalent, encompassing conditions such as anxiety, depression, and inertia (12, 13). Taken together, cognitive and psychological symptoms can profoundly influence rehabilitation outcomes, often reducing treatment adherence and limiting patient activity, participation, and functional improvements (14). In response to these complexities, rehabilitation has increasingly embraced a broader perspective, incorporating non-motor domains into recovery processes. Studies have highlighted that RAT, particularly when integrated with supplementary systems (e.g., virtual reality [VR], wearable devices, functional electrical stimulation [FES], Brain–Computer Interface [BCI]), can enhance conventional training by offering a combined approach to post-stroke rehabilitation (15–17).
Nevertheless, despite the promising advancements in RAT over the last 2 decades, its integration into routine clinical practice remains limited due to a persistent gap between technological innovation and its standardized adoption within rehabilitation settings (3, 18), representing a key conceptual challenge in the current landscape of post-stroke rehabilitation. Moreover, while RAT has widely demonstrated its efficacy in motor recovery, recent literature still highlights the need for a deeper study of its widespread impact on non-motor dimensions (19), as evidence on QoL, cognitive, and psychosocial outcomes remains fragmented and often derives from secondary or exploratory analyses rather than being the primary focus of intervention trials. In addition, previous studies report substantial heterogeneity in outcome measures, intervention characteristics, and follow-up assessment, limiting the comparability of findings and the generalizability of conclusions across non-motor domains (9, 14, 17, 19). These gaps underscore the need for a systematic evaluation and synthesis of the broader effects of RAT to align its application with emerging patient-centred and technology-enabled healthcare models.
Following this line, the present work aimed to systematically review the available literature investigating the effects of RAT on post-stroke non-motor outcomes, namely QoL, cognition, and psychosocial functioning. Specifically, intervention procedures and metrics adopted to estimate RAT effects were summarized to provide future studies and rehabilitation practice with clearer evidence. Also, both short- and long-term effects were analysed to shed light on RAT’s lasting benefits and potentially inform future practices in post-discharge programmes.
Methods
Preliminary checks on registered or ongoing similar literature reviews and/or meta-analyses were carried out through the International Prospective Register of Systematic Review (PROSPERO) platform. The search provided no results and, thus, the systematic review protocol was registered (ref. CRD42024594665).
Search strategy and studies selection
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (20) were followed throughout the entire review process. Preliminary electronic searches were performed on the 28 June 2024 from Web of Science, PubMed, Cochrane Library, CINAHL, Embase, and PsycINFO by applying the following search query: (rehabilitation) AND (stroke) AND ((robot*) OR (exoskelet*) OR (end-effector)) AND ((quality of life) OR (cogn*) OR (psych*) OR (well-being)). The use of general search terms as “rehabilitation” or “psych*” was preferred to ensure wider retrieval and select eligible records via a manual check along screening procedures. Eligibility criteria were defined a priori according to the PICOS framework, as follows: (P) adult patients with ischaemic or haemorrhagic stroke; (I) RAT delivered to upper and/or lower limbs, including exoskeletons, end-effector systems, and/or soft-robotic devices, either alone or coupled with supplementary systems (e.g., VR, FES, BCI); (C) Usual care, conventional rehabilitation, other technology-assisted interventions, or no-treatment control conditions; (O) post-stroke non-motor outcomes, namely QoL, cognitive functioning, and psychosocial variables; (S) experimental and observational study designs, including randomized controlled trials (RCTs), non-RCTs, before–after studies, and cohort studies. Moreover, additional filters (e.g., English language, original peer-reviewed research, year of publication timespan) were applied across electronic databases to optimize and refine the identification of the studies. In addition, the reference lists of all included full-text articles were manually screened to identify further relevant studies potentially missed by electronic search. A reference management system (HubMeta) (21) was used to import, find, and remove duplicates, and screen the records identified iteratively.
Risk of bias assessment
All records included were evaluated based on their study design using the National Institutes of Health (NIH) Quality Assessment Tools for Controlled Intervention Studies (14 items), for Before–After (Pre–Post) Studies with No Control Group (12 items), and for Observational Cohort and Cross-Sectional Studies (14 items) (22). These included questions assessing criteria that ranged from study enrolment and evaluation (e.g., randomization, allocation, eligibility criteria, blinding, outcome measures validity) to intervention and analysis procedures (e.g., dropout management, adherence to treatment, power calculation, statistical analyses appropriateness). For all checklists, each item was rated as “yes” (1 point), “no” (0 points) or “not applicable”, resulting in a total score that was classified in terms of methodological quality as “Poor” (< 50%), “Fair” (50–75%), or “Good” (> 75%). Details on each tool’s questions and scoring procedures are reported as Supplementary material. Three researchers (FZ, LF, ST) evaluated all studies working independently and any discrepancies were discussed until full consensus was reached. The studies with lower scores (i.e., higher risk of bias) were not excluded from final synthesis, but their methodological quality was considered in interpretation of the findings (23).
Data extraction and synthesis
According to eligibility criteria, progressive exclusion of non-eligible records was performed through screening procedures starting from the titles and abstracts, and then checking for the full texts. The entire review process was completed by 3 authors (FZ, LF, ST) blinded to one another’s studies classification. Disagreements on records exclusion were discussed and solved through planned periodical meetings with the entire research group aimed at reaching a consensus. At the full-text screening stage, each article identified was read multiple times to ensure a full understanding of the study aim, design, outcomes investigated, and findings. A wide range of data was then extracted from the studies included. These were collected in a synoptic table (see Supplementary material), which in detail includes: author(s), year of publication, country where the study was conducted and related Human Development Index (HDI) and rank (24), study design (including if pilot, funded, multicentre, and/or longitudinal), patients’ characteristics (i.e., type of hospitalization, stroke aetiology and onset, sample size, mean age, sex distribution, and ethnicity), RAT characteristics and delivery modalities (i.e., robotic device typology and name, targeted extremities, use of any supplementary device, overall trial duration, total number of RAT session and duration, and comparator(s)), study outcomes along with the metrics adopted (i.e., both motor and non-motor domains), and main results found. Descriptive statistics were computed on the main characteristics of the studies (i.e., means, standard deviations, percentages), while the results were meta-synthetized through a narrative approach. No statistical software or tool was employed for data analysis and synthesis.
Results
Studies selection
At initial electronic search, a total of 1,963 records were retrieved. After duplicates removal, 1,388 records were screened by title and abstract. Two additional records were retrieved from abstract screening and added manually, for a total of 141 remaining articles that were screened by full text. Of these, 90 met all eligibility criteria and underwent data extraction. The review process and studies selection along with the reasons for exclusion at each screening stage are showed in Fig. 1. Most of the records excluded were labelled as off-topic (n = 309), included no non-motor outcomes (n = 434) or belonged to grey literature (n = 397). Others involved samples of paediatric patients or other clinical populations (n = 145), while fewer studies were excluded for language reasons (n = 11) or because the abstract or the full text was not available (n = 4).

Risk of bias
The Controlled Intervention Studies checklist was used to evaluated both randomized controlled trials (RCTs) and non-randomized controlled studies (n = 61). The evaluation differed between the 2 study designs only for the items specifically referring to randomization procedures (items 1 to 3) and intention-to-treat analysis (item 14) criteria. These were labelled as “not applicable” for non-randomized controlled studies and were not counted for total scoring and subsequent quality rating. Overall, of the RCTs (n = 53), an equal distribution was observed between “Good” (n = 26, 49.1%) and “Fair” (n = 26, 49.1%) studies, with only 1 trial labelled as “Poor” (1.8%). Similarly, half of the non-randomized studies were rated as “Good”, the other half as “Fair” (n = 4, 50%). Regarding the Before–After (Pre–Post) studies with no control group (n = 10), most were classified as “Fair” (n = 8, 80%), whereas only 2 studies reached “Good” methodological quality (20%). Lastly, the Observational Cohort and Cross-Sectional Studies assessment tool was used to evaluate retrospective cohort studies (n = 19). The majority were rated as having “Fair” quality (n = 11, 57.9%), and fewer were classified as “Good” (n = 8, 42.1%).
Overall, satisfactory levels of methodological quality were observed across all the studies included. Only a small number (i.e., 11.1%) were rated as “Poor” or were at the lower marginal limits of “Fair” classification, thus potentially having a higher risk of bias. Across study designs, most recurrent methodological concerns regarded the absence of blinding of patients, treatment providers, and outcome assessors, the lack of a priori sample size or power calculations, the absence of stratified analysis exploring dose–response relationship, and the limited consideration of potential confounding factors. None of the studies included satisfied all evaluation criteria in any of the tools adopted. For each study, details on the evaluation are provided as Supplementary material.
Characteristics of the studies included
All data extracted from the studies included are presented in a synoptic table (see Supplementary material) (25–114).
Design and participants
The main characteristics and the design of the studies included are presented in Tables I and II. Almost half of the studies were published within the last 5 years (n = 43, 47.8%) and conducted in European countries (n = 44, 48.9%). In particular, most were from countries classified as having “very high” (86.7%) or “high” (12.2%) human development, according to the latest United Nations HDI rank. Regarding the design, the majority of conducted RCTs (58.9%), were single-centred (77.8%) and received funding (51.1%). Fewer studies were pilot (18.9%) and included follow-up evaluations (30.0%), which mainly lasted less than 6 months (59.3%, follow-up range: 2 weeks–72 months).
| Year of publication | n (%) | Nationa | n (%)b | HDI rankc | n (%) |
| 2021–2024 | 43 (47.8) | Europe | 44 (48.9) | Very high | 78 (86.7) |
| 2016–2020 | 31 (34.4) | Asia | 33 (36.7) | High | 11 (12.2) |
| 2000–2015 | 16 (17.8) | America | 13 (14.4) | Medium | 1 (1.1) |
| Oceania | 1 (1.1) | Low | – | ||
| aEurope (i.e., Lithuania, Italy, Austria, Germany, Sweden, France, Belgium, Czech Republic, Netherlands, United Kingdom, Switzerland, Spain, Romania), America (i.e., Canada, United States of America), Asia (i.e., China, South Korea, Japan, Turkey, Taiwan, Russia, India), Oceania (Australia). bNon-cumulative percentage. cThe Human Development Index (HDI) is a composite score accounting for (i) life expectancy at birth, (ii) expected years of schooling and mean years of schooling, and (iii) Gross National Income per capita. Rank categorization is based on 2023–2024 United Nations Development Programme Report, https://hdr.undp.org/ (accessed November 1, 2024). | |||||
Of the participants involved (Table III), most were inpatients (n = 62, 68.9%) and were diagnosed with ischaemic or haemorrhagic stroke (n = 72, 80.0%). Overall, a total of 6,521 patients were included. Some 26.7% of the studies (n = 24) included less than 30 participants (range: 7–770). Moreover, the majority involved samples aged on average under 65 years (n = 62, 68.9%) and were mostly composed of men (i.e., ≥ 60.0%; n = 66, 73.3%). Only 2 studies reported participants ethnicity.
Intervention
The types of robotic devices used along with the main characteristics of the interventions are summarized in Table IV. Most of the included studies implemented exoskeletal devices (n = 48, 53.3%) followed by the use of end-effectors (n = 38, 42.2%) for targeting either upper (48.9%) or lower (50.0%) limb function recovery. The intervention period varied widely across the studies in terms of overall duration (range: 2–52 weeks), total number of sessions (range: 2–60), and session duration (20–240 min). Of the studies with control conditions, intervention effects were compared with patients assigned to usual care (n = 50, 63.3%) or other technology-assisted training or procedures (e.g., VR-based therapy, passive robotic intervention; different robotic device; n = 21, 36.7%). Of the total, 11 studies (12.2%) implemented supplementary devices in combination with RAT as experimental condition (i.e., functional and neuromuscular electrical stimulation, brain–computer interface systems, non-immersive VR devices, cycle ergometer, bodyweight support system-integrated treadmill).
Outcomes
A summary of the non-motor outcomes and domains investigated is reported in Table V. These were evaluated through standardized measures intended to profile patients’ QoL, cognition, and psychosocial functioning, which were conceptualized in the present review as interrelated components of post-stroke global functioning, reflecting patients’ emotional, cognitive, behavioural, and social adaptation to daily activity and participation after stroke. Regarding QoL evaluation (n = 46, 51.1%), a wide range of sub-domains were investigated and, in the present review, classified as a measure of well-being, based on emotional (e.g., mood, role limitations due to emotional problems), physical (e.g., energy, fatigue), cognitive (e.g., memory, communication), or social (e.g., participation, work/productivity) factors, thus capturing patients’ perceived functioning across multiple life areas. As for cognitive functioning (n = 43, 47.8%), most of the studies conducted comprehensive evaluations on global cognition, while others assessed selected cognitive domains like executive functions, attention, memory, visuo-spatial abilities, and/or intelligence and reasoning, which underpin patients’ capacity to plan, adapt, and effectively engage in rehabilitation and daily activities. Of the studies including psychosocial variables (n = 37, 41.1%), most evaluated patients’ anxiety and/or depression symptoms, while the remaining specifically estimated intervention changes on perceived self-efficacy, fear of falling, psychological well-being, fatigue, coping strategies, and motivational factors, all of which reflect emotional regulation, personal resources, and psychological adjustment within the broader framework of global functioning. Outcome metrics for each study domain are summarized in Fig. 2.
| QoLa | n (%)b | Cognition | n (%)b | Psychosocial | n (%)b | |
| Emotional well-being | 32 (35.5) | Global functioning | 32 (35.5) | Anxiety/Depression | 29 (32.2) | |
| Physical well-being | 20 (22.2) | Attention | 9 (10.0) | Self-efficacy | 5 (5.5) | |
| Cognitive well-being | 30 (33.3) | Executive functions | 14 (15.5) | Fear of falling | 5 (5.5) | |
| Social well-being | 36 (40.0) | Memory | 5 (5.5) | Psychological well-being | 4 (4.4) | |
| Visuo-spatial abilities | 3 (3.3) | Fatigue | 3 (3.3) | |||
| Intelligence | 1 (1.1) | Treatment perception | 3 (3.3) | |||
| Coping | 2 (2.2) | |||||
| Motivation | 1 (1.1) | |||||
| Personality traits | 1 (1.1) | |||||
| aEmotional well-being (SF Health Survey – role limitation due to emotional problems, emotional well-being; SIS – emotion; SS-QoL – mood, personality; WHOQOL-BREF – psychological domain); Physical well-being (SS-QoL – energy, SF Health Survey – energy/fatigue; role limitation to physical problems; NHP – energy); Cognitive well-being (SS-QoL – language, thinking; SIS – memory, communication); Social well-being (SS-QoL – family roles, social roles, work/productivity; WHOQOL-BREF – social domain, environmental domain; SF Health Survey – social functioning; SIS – social participation). Treatment perception includes outcomes related to intervention expectations, perceived effectiveness and recovery locus of control. bNon-cumulative percentages. |
||||||
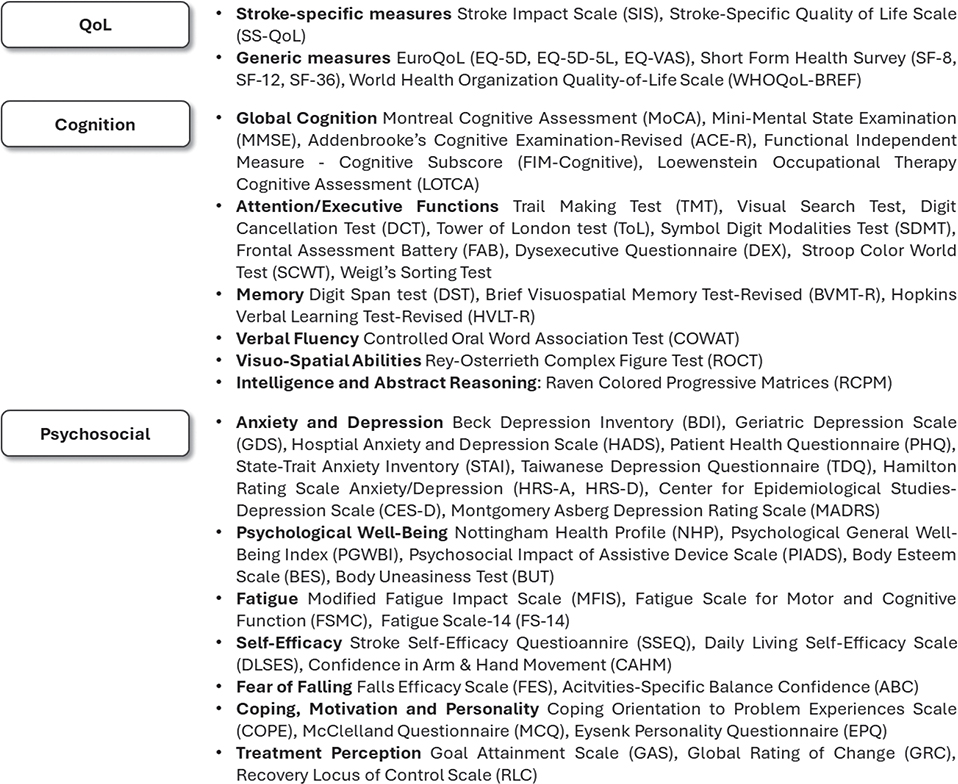
Fig. 2. Summary of the non-motor outcome measures adopted in the studies included.
RAT effects on QoL
More than the half of the studies including QoL outcomes reported significant changes following RAT (n = 29, 63.0%), while fewer reported null effects (n = 17, 37.0%). Significant improvements were found in the subdomains of emotional (27, 33, 46, 58, 61, 70, 80–83, 85, 92, 102, 112), physical (27, 46, 54, 61, 70, 80, 82), cognitive (27, 33, 46, 58, 70, 80–83, 92, 112), and social (27, 33, 44, 46, 58, 61, 68, 70, 80–83, 85, 87, 92, 102, 103, 105, 106, 112) well-being, with some studies also reporting wider changes than a control group exposed to usual care (27, 33, 44, 54, 70, 80, 82, 85) or alternative therapy (46, 58, 68, 82, 87). On average, the overall duration of RAT in the studies estimating significant effects was on average 8 weeks (range: 3–48 weeks) and mainly deployed exoskeletal devices. Moreover, most studies assessed patients who initiated the intervention within 6 months after stroke onset (68, 4%) and included follow-up evaluation with varying duration (range: 1 month–6 years from RAT completion). Only 8 studies found significant longitudinal effects (26, 33, 44, 58, 85, 88, 102, 103). Of these, follow-up duration was up to 12 months and reported on all well-being subdomains.
RAT effects on cognition
Most of the studies investigating RAT’s impact on cognitive outcomes found significant improvements (n = 26, 76.5%). Among these, most observed significant post-intervention changes on global cognition (25, 39, 41, 45, 63, 65, 76, 78, 97, 101, 104, 110, 113, 114), followed by within-subject effects on executive functions (31, 37, 56, 62, 69, 76, 78, 101), attention (25, 31, 37, 56, 78), visuo-spatial abilities (25, 31, 101), memory (25, 31), and intelligence (36). Additionally, 10 studies showed that RAT was significantly superior in targeting these outcomes compared with standard care (36, 37, 41, 45, 65, 78, 101) or other training methods (i.e., VR-based training, alternative robotic devices, gait training with orthoses) (25, 78, 96, 114). Overall, RAT duration ranged from 2 to 8 weeks, primarily using end-effector or exoskeleton devices coupled to non-immersive VR exposure. More than the half of the studies (60.0%) included patients who had experienced stroke 6 months prior to the intervention. Only 2 studies (73, 90) conducted follow-up evaluations at 4 and 8 -months following RAT, respectively, and neither found significant long-term effects.
RAT effects on psychosocial outcomes
Approximately half of the studies investigating RAT’s impact on psychosocial outcomes reported significant effects (n = 18, 52.9%), while the other half did not. At post-intervention, significant within-group improvements were observed in anxiety or depression symptoms (35, 42, 51, 67, 72, 76, 78, 79, 88, 93, 98, 100, 111), psychological well-being (35, 42, 48, 76), coping strategies (35, 42), self-efficacy (38, 50, 100), fear of falling (88), and perceived fatigue (37, 51). Fewer studies reported significant group interaction effects, suggesting RAT to be more effective than standard training controls (42, 50, 51, 79, 85, 88, 98, 111). RAT overall duration ranged from 2 to 8 weeks and mainly employed the use of exoskeletons without any supplementary devices. Most of the studies included patients affected by stroke within the last 6 months (56.3%). Only 2 of them (67, 85) conducted follow-up evaluations (up to 4 months), but no significant effects over time were reported on psychological outcomes.
Non-motor correlates of RAT effectiveness
Some of the studies included in data synthesis investigated the role of selected non-motor variables as covariates or predictors of patient recovery. Among these, significant correlations were found between motor improvement and global cognition (74, 77, 101), executive functions (29, 55, 93), attention (29), and visuo-spatial abilities (93). Specifically, 2 studies showed that global cognition at baseline significantly predicted increased patient autonomy (71, 77), whereas others reported no significant impact over the trial period (32, 89, 97). Similarly, significant associations were estimated with self-efficacy (75, 100), locus of control (34), depression (100), and anxiety (34) symptoms, which significantly predicted better rehabilitation outcomes.
DISCUSSION
The present review aimed to systematically summarize the studies that investigated the efficacy of RAT on non-motor outcomes in patients affected by stroke. Specifically, from each study included, the effects on QoL, cognition, and psychosocial outcomes were extracted and meta-synthesized, with the final purpose of providing an overview of the widespread impact of robotics in post-stroke rehabilitation programmes.
At screening process completion, a total of 90 studies were analysed. Of these, most were published over the past 10 years with a notable increase in the last 5, indicating rapid and growing attention on using RAT to target a wider range of post-stroke outcomes besides motor functioning. Such interest has spanned multiple countries worldwide, particularly those at higher HDI levels. This not only reflects limited use of robotics in less developed countries, but also underscores the need to promote more equitable access. Given the global rise in stroke cases projected over the coming decades (2, 115), fostering wider accessibility to robotic technologies could be crucial. In light of this, considering also the higher costs associated with technology implementation compared with traditional treatments (more than the half of the studies included were funded), future research on RAT should integrate cost-effectiveness data into their analyses, thereby enriching the literature with additional insights for improved economic considerations. Beyond this, wider accessibility to robotic technologies may also be particularly relevant from a rehabilitation perspective. RAT allows the delivery of training with precision and consistency that is harder to achieve with conventional therapy alone. Among the advantages are high intensity, repetition, and task-specificity along with objective control and enriched sensorimotor feedback. These features may be especially valuable for patients with severe impairments or limited voluntary movement, for whom standard treatment can be less effective or more difficult to individualize.
Regarding the methodological characteristics of the studies included, heterogeneous and mixed data were synthetized. Although most of the works adopted an RCT design, many others reported retrospective cohort observations, did not perform randomization, or tested the efficacy of RAT with no control groups. Moreover, most were single-centred, did not schedule follow-up evaluations, and involved patients affected by stroke of different aetiology and varying time of onset. Sample size also varied extensively. Although a considerable number of patients were included in this review, 1 study in 4 involved less than 30 participants, often leading to statistically underpowered evidence. Furthermore, most patients were men and aged under 65 years. Although such distribution aligns with the global trends observed over the past 2 decades (i.e., among people younger than 70 years, prevalence and incidence rates increased by 22% and 15% respectively; males experienced a greater burden of disease in terms of DALYs compared with females) (116), this configuration constrains the drawing of conclusions concerning RAT’s effectiveness across other demographic groups, such as older adults and females. Lastly, only 2 studies reported participants’ ethnicity, which results in additional lack of informative data for findings’ replicability and applicability, as suggested in a prior study (117). Taken together, despite the heterogeneity observed, the overall methodological quality of the studies included was judged as satisfactory. Based on the risk-of-bias evaluation undertaken, more rigorous randomization methods, allocation concealment, blinding procedures, and intention-to-treat analyses are encouraged for future RCTs, when applicable. Also, analysing individual-level data along with the adoption of interrupted time-series designs is recommended for future studies with no control group to further increase results confidence and analysis sensitivity. Furthermore, future observational cohort studies should more accurately identify and measure key potential confounding variables so as to better investigate their impact on the relationship between RAT exposure and rehabilitation outcomes over time.
Further heterogeneity was found regarding the intervention characteristics. Despite the studies included being equally distributed for the use of device typology (exoskeleton or end-effector) and for targeted extremities (upper or lower) and related functions, the duration of the rehabilitation programmes varied widely in terms of total number of sessions and each session’s duration. These data reflect the broader and ongoing debate regarding the definition of treatment dosage. While it is acknowledged that training intensity can significantly impact post-stroke neural reorganization and rehabilitation outcomes, the optimal dosage threshold has not yet been established (118, 119). So far, the use of robotic technology has been considered valuable to increase the amount of therapy, as it allows better research into treatment dosage through more precise and quantifiable control of therapy (17). In the present review, across the data extracted, no clear and repeated patterns were found, showing that longer or more intensive interventions were linked to increased effectiveness across outcome domains. However, future meta-analyses should further address this association to better inform the dose–response relationship and seek proper treatment intensity for patients, specifically in targeting non-motor outcomes. Moreover, very few studies among those included investigated the role of treatment intensity or timed initiation as covariates of non-motor change. Further work in this direction is warranted. Following this line, future research should also adopt more theory-driven and mechanistic approaches to better clarify the potential transfer effects of RAT on non-motor outcomes. Standardized protocols and systematic manipulation of specific treatment components (e.g., task demands, feedback modalities) are needed to provide deeper insights into how different robotic deployments may differentially affect the non-motor recovery process.
Multiple outcome domains and measures were retrieved and synthetized. Moreover, intervention effects were examined with reference to the trial design and participants’ characteristics. Notably, all studies adopted standardized metrics, which ensured increased validity of the data collected across the different interventions. Of those assessing changes on QoL, both generic and stroke-specific tools were used. Widespread effects were observed on various aspects of perceived well-being, including emotional, physical, cognitive, and social sub-domains. These mainly provided encouraging evidence on the immediate impact of RAT (resulting in some cases being superior to standard training), while only a smaller proportion of studies supported the long-term effects after the intervention (up to 12 months). These findings corroborate what emerged from a prior systematic review on QoL changes following RAT (9), which supported its integration into conventional treatments but reported limited longitudinal evidence especially among individuals with stroke, despite this being the most investigated neurological population. Accordingly, further follow-up research is encouraged to enrich the literature with longitudinal evidence and draw more robust conclusions concerning RAT’s effects on perceived well-being over time. Moreover, the high variability observed in participants’ stroke aetiology and time since first onset made it difficult to identify possible clinical determinants of RAT efficacy on QoL. Future studies involving larger and more clinically homogeneous samples are recommended. Contextually, performing more in-depth cluster analyses and targeting selected well-being sub-domains would also be informative.
Regarding the studies focusing on cognitive outcomes, batteries of standardized tests were used. Pre–post intervention evaluations included global cognition, attention, executive functions, memory, visuo-spatial abilities, and intelligence. Again, significant changes following RAT were observed across all cognitive domains, with some studies showing the integration of robotics to provide wider improvements compared with traditional treatments. This finding confirms the potential of robotic technology to promote neuroplasticity and, simultaneously, provide cognitive stimulation. It is widely acknowledged that motor recovery not only relates to the motor processes but also to the sensory and proprioceptive systems, which share mutual neural circuits and influence each other during training (120, 121). By increasing treatment intensity, repeatability, and optimization, RAT enables augmented motor inputs from peripheral joints, ultimately providing task-specific stimulation to the central nervous system and a concurrent impact on cognitive functioning (122, 123). Moreover, most of the included studies combined the use of robotics with VR devices, which further enhanced patients’ exposure to multimodal and multisensory stimuli. Accordingly, the interaction with visual feedback or virtual games coupled to robot-assisted reaching, grasping, or walking improved dual-task training, which in turn facilitated the activation of the neuroplastic processes involved in the recovery of both motor and cognitive functions. Accordingly, future trials are encouraged to leverage the combination of RAT and VR. Despite being promising, however, it must be noted that the results synthetized were extracted mainly from studies including clinically mixed and small samples and describing interventions of varying durations. Additionally, none of them reported significant effects over time. Future full-scale and standardized intervention studies including more extended follow-up evaluations are recommended to better clarify the longitudinal benefits of RAT on cognition.
Finally, of the psychosocial outcomes included, a wide range of domains were investigated, namely depression and anxiety levels, self-efficacy, fear of falling, psychological well-being and fatigue, and coping strategies. Similarly to previous outcomes, significant effects were found following RAT across almost all outcomes, with major evidence on depression and anxiety changes. Other work also focused on the moderating or predictive role of motivational factors, perceived locus of control, and personality traits to impact rehabilitation outcomes, but mixed or inconclusive results were found. Interestingly, most of the studies that reported a positive psychological impact also evidenced significant improvements in motor and functional status. While this finding suggests that RAT may be effective for non-motor outcomes, evidence on the relationship between motor and psychological change was limited. This makes it difficult to determine whether the psychological benefits were secondary to motor improvement or a direct result of RAT exposure. In general, the psychosocial benefits resulting from neurorehabilitation processes are increasingly recognized, especially when multidisciplinary approaches are adopted (124, 125). Additional studies investigating the integration of robotics into standard training along with multi-domain network analyses are recommended to better outline the widespread impact of RAT. Furthermore, even in studies investigating psychosocial outcomes, the interventions varied widely in total duration and dosage intensity, with a predominant use of exoskeletons. Moreover, most of the patients involved had stroke onset within 6 months and, at RAT completion, were evaluated only up to 4 months, with no significant longitudinal effects being reported. Future studies with standardized intervention parameters are suggested to identify optimal protocols for RAT additionally targeting psychosocial outcomes. Extending follow-up periods and exploring RAT’s impact in later stroke stages is also crucial to determine long-term effects and broader applicability.
Limitations and directions for future research
Overall, the studies included in this systematic review allow for the description of informative and encouraging evidence on robotic devices’ application to post-stroke rehabilitation programmes, especially the impact on non-motor outcomes. However, some limitations should be acknowledged. First, despite the relatively large number of studies identified, no meta-analysis was conducted. This choice was driven by the substantial heterogeneity observed across studies in terms of design, participants’ profile, intervention features, and outcome domains and measures, which precluded a reliable quantitative synthesis. Such variability also made it difficult to draw robust conclusions and represents the main limitation of the present review. Outcome-specific in-depth analyses along with the implementation of more adaptive RAT trial protocols are highly recommended for future studies. In addition, in most of the included studies non-motor outcomes were not defined as primary endpoints but instead assessed as secondary or exploratory measures. This may have resulted in limited statistical power, thereby constraining the findings’ interpretability and generalizability. Future research should prioritize more rigorous methodological designs (e.g., improved randomization, blinding, and longitudinal follow-up), larger and more clinically homogeneous samples, and extend follow-up periods to clarify dose–response relationships, long-term effects, and applicability across different stroke stages. Also, theory-driven and mechanistic studies manipulating key intervention components are needed to elucidate the transfer of RAT onto non-motor outcomes (as primary endpoints). Integrating cost-effectiveness analyses and adopting a more integrative, multi-domain, and network-based approach will be essential to advance personalized, patient-centred rehabilitation pathways and inform future clinical implementation. Also, the adoption of longitudinal designs is warranted. Prospective data would better inform RAT effectiveness through multiple observations, ultimately highlighting outcomes’ long-term trajectories and the role of potential correlates over time. In conclusion, future research should also adopt more integrative approaches. Besides motor functions, the assessment of QoL, cognitive, and psychosocial outcomes within the same intervention protocol would allow for more comprehensive evaluations of the multi-domain impact of RAT. This method would better address post-stroke global functioning, identify potential recovery profiles, and ultimately promote the development and implementation of individualized, patient-centred rehabilitation pathways.
Conclusions
RAT shows promising effects beyond post-stroke motor recovery, potentially improving non-motor outcomes such as QoL, cognition, and psychosocial functioning. However, substantial heterogeneity limited generalizable conclusions, calling for more rigorous, complex, and theory-driven studies with long-term follow-up to better clarify mechanisms, effectiveness, and clinical implementation.
ACKNOWLEDGEMENTS
Ethics approval and consent to participate
The present work is part of a broader research protocol entitled ITER Project – Users’ experience and cognitive Improvement in high-TEchnology Rehabilitation programmes for post-stroke patients. A multi-method, multi-informant, patient-centred approach – approved by the Territorial Ethics Committee – Lombardy (6 May 2024, Prot. N. 0025654/24). Consent to participate is not applicable.
REFERENCES
- Steinmetz JD, Seeher KM, Schiess N, Nichols E, Cao B, Servili C, et al. Global, regional, and national burden of disorders affecting the nervous system, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet Neurol 2024; 23: 344-381. https://doi.org/10.1016/S1474-4422(24)00038-3
- Pu L, Wang L, Zhang R, Zhao T, Jiang Y, Han L. Projected global trends in ischemic stroke incidence, deaths and disability-adjusted life years from 2020 to 2030. Stroke 2023;5: 1330-1339. https://doi.org/10.1161/STROKEAHA.122.040073
- Alt Murphy M, Pradhan S, Levin MF, Hancock NJ. Uptake of technology for neurorehabilitation in clinical practice: a scoping review. Phys Ther 2024; 104: pzad140. https://doi.org/10.1093/ptj/pzad140
- Molteni F, Gasperini G, Cannaviello G, Guanziroli E. Exoskeleton and end-effector robots for upper and lower limbs rehabilitation: narrative review. PM & R 2018; 10(9S2). https://doi.org/10.1016/j.pmrj.2018.06.005
- Iandolo R, Marini F, Semprini M, Laffranchi M, Mugnosso M, Cherif A, et al. Perspectives and challenges in robotic neurorehabilitation. Appl Sci 2019;9: 3183. https://doi.org/10.3390/app9153183
- Giansanti D. The rehabilitation and the robotics: are they going together well? Healthcare 2020; 9: 26. https://doi.org/10.3390/healthcare9010026
- Calabrò RS, Sorrentino G, Cassio A, Mazzoli D, Andrenelli E, Bizzarini E, et al. Robotic-assisted gait rehabilitation following stroke: a systematic review of current guidelines and practical clinical recommendations. Eur J Phys Rehabil Med 2021; 57. https://doi.org/10.23736/S1973-9087.21.06887-8
- Morone G, Palomba A, Martino Cinnera A, Agostini M, Aprile I, Arienti C, et al. Systematic review of guidelines to identify recommendations for upper limb robotic rehabilitation after stroke. Eur J Phys Rehabil Med 2021; 57: 238-245. https://doi.org/10.23736/S1973-9087.21.06625-9
- Zanatta F, Farhane-Medina NZ, Adorni R, Steca P, Giardini A, D’Addario M, et al. Combining robot-assisted therapy with virtual reality or using it alone? A systematic review on health-related quality of life in neurological patients. Health Qual Life Outcomes 2023;21: 18. https://doi.org/10.1186/s12955-023-02097-y
- Sun JH, Tan L, Yu JT. Post-stroke cognitive impairment: epidemiology, mechanisms and management. Ann Transl Med 2014; 2: 80.
- Jokinen H, Melkas S, Ylikoski R, Pohjasvaara T, Kaste M, Erkinjunttiet T, al. Post-stroke cognitive impairment is common even after successful clinical recovery. Eur J Neurol 2015; 22: 1288-1294. https://doi.org/10.1111/ene.12743
- Devereux N, Berns AM. Evaluation & treatment of psychological effects of stroke. Del J Public Health 2023;9: 62-69. https://doi.org/10.32481/djph.2023.08.011
- Hackett ML, Köhler S, O’Brien JT, Mead GE. Neuropsychiatric outcomes of stroke. Lancet Neurol 2014; 13: 525-534. https://doi.org/10.1016/S1474-4422(14)70016-X
- Park JG. Update on stroke rehabilitation for non-motor impairment. Brain Neurorehabil 2022; 15: e13. https://doi.org/10.12786/bn.2022.15.e13
- Reis SB, Bernardo WM, Oshiro CA, Krebs HI, Conforto AB. Effects of robotic therapy associated with non-invasive brain stimulation on upper-limb rehabilitation after stroke: systematic review and meta-analysis of randomized clinical trials. Neurorehabil Neural Repair 2021; 35: 256-266. https://doi.org/10.1177/1545968321989353
- Qu Q, Lin Y, He Z, Fu J, Zou F, Jiang Z, et al. The effect of applying robotassisted task-oriented training using human-robot collaborative Interaction Force Control Technology on Upper Limb Function in Stroke Patients: Preliminary Findings. BioMed Res Int 2021; 2021. https://doi.org/10.1155/2021/9916492
- Rajashekar D, Boyer A, Larkin-Kaiser KA, Dukelow SP. Technological Advances in stroke rehabilitation. Phys Med Rehabil Clin N Am 2024; 35: 383-398. https://doi.org/10.1016/j.pmr.2023.06.026
- Proietti T, Ambrosini E, Pedrocchi A, Micera S. Wearable robotics for impaired upper-limb assistance and rehabilitation: state of the art and future perspectives. IEEE Access 2022;10: 106117-106134. https://doi.org/10.1109/ACCESS.2022.3210514
- Walker MF, Hoffmann TC, Brady MC, Dean CM, Eng JJ, Farrinet AJ, al. Improving the development, monitoring and reporting of stroke rehabilitation research: consensus-based core recommendations from the Stroke Recovery and Rehabilitation Roundtable. Int J Stroke 2017; 12: 472-479. https://doi.org/10.1177/1747493017711815
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. Published online March 29, 2021: n71. https://doi.org/10.1136/bmj.n71
- Steel P, Fariborzi H, Hendijani R. An application of modern literature review methodology: finding needles in evergrowing haystacks. New York: SAGE Publications; 2023. https://doi.org/10.4135/9781529667417
- National Heart, Lung, and Blood institute. Study quality assessment. Available from: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools
- Stone J, Gurunathan U, Glass K, Munn Z, Tugwell P, Doi SAR. Stratification by quality induced selection bias in a meta-analysis of clinical trials. J Clin Epidemiol 2019; 107: 51-59. https://doi.org/10.1016/j.jclinepi.2018.11.015
- Human Development Report. Human Development Index and its components (accessed November 2024). Available from: https://hdr.undp.org/data-center/human-development-index#/indicies/HDI
- Adomavičienė A, Daunoravičienė K, Kubilius R, Varžaitytė L, Raistenskis J. Influence of new technologies on poststroke rehabilitation: a comparison of Armeo Spring to the Kinect System. Med Kaunas Lith 2019; 55. https://doi.org/10.3390/medicina55040098
- Ahn SY, Bok SK, Lee JY, Ryoo HW, Lee HY, Park HJ, et al. Benefits of robot-assisted upper-limb rehabilitation from the subacute stage after a stroke of varying severity: a multicenter randomized controlled trial. J Clin Med 2024; 13. https://doi.org/10.3390/jcm13030808
- Akinci M, Burak M, Kasal FZ, Özaslan EA, Huri M, Kurtaran ZA. The effects of combined virtual reality exercises and robot assisted gait training on cognitive functions, daily living activities, and quality of life in high functioning individuals with subacute stroke. Percept Mot Skills 2024;131: 756-769. https://doi.org/10.1177/00315125241235420
- Ambrosini E, Gasperini G, Zajc J, Immick N, Augsten A, Rossini M, et al. A robotic system with EMG-triggered functional electrical stimulation for restoring arm functions in stroke survivors. Neurorehabil Neural Repair 2021; 35: 334-345. https://doi.org/10.1177/1545968321997769
- Aprile I, Guardati G, Cipollini V, Papadopoulou D, Monteleone S, Redolfi A, et al. Influence of cognitive impairment on the recovery of subjects with subacute stroke undergoing upper limb robotic rehabilitation. Brain Sci 2021; 11. https://doi.org/10.3390/brainsci11050587
- Aprile I, Germanotta M, Cruciani A, Pecchioli C, Loreti S, Papadopoulou D, et al. Poststroke shoulder pain in subacute patients and its correlation with upper limb recovery after robotic or conventional treatment: a secondary analysis of a multicenter randomized controlled trial. Int J Stroke 2021; 16: 396-405. https://doi.org/10.1177/1747493020937192
- Aprile I, Guardati G, Cipollini V, Papadopoulou D, Mastrorosa A, Castelli L, et al. Robotic rehabilitation: an opportunity to improve cognitive functions in subjects with stroke: an explorative study. Front Neurol 2020; 11. https://doi.org/10.3389/fneur.2020.588285
- Bergqvist M, Möller MC, Björklund M, Borg J, Palmcrantz S. The impact of visuospatial and executive function on activity performance and outcome after robotic or conventional gait training, long-term after stroke as part of a randomized controlled trial. PloS One 2023; 18: e0281212. https://doi.org/10.1371/journal.pone.0281212
- Bhattacharjee S, Barman A, Patel S, Sahoo J. The combined effect of robot assisted therapy and activities of daily living training on upper limb recovery in persons with subacute stroke: a randomized controlled trial. Arch Phys Med Rehabil. Published online 2024. https://doi.org/10.1016/j.apmr.2024.01.027
- Bragoni M, Broccoli M, Iosa M, Morone G, De Angelis D, Venturiero V, et al. Influence of psychologic features on rehabilitation outcomes in patients with subacute stroke trained with robotic-aided walking therapy. Am J Phys Med Rehabil 2013; 92: e16-25. https://doi.org/10.1097/PHM.0b013e3182a20a34
- Calabrò R, De Cola M, Leo A, et al. Robotic neurorehabilitation in patients with chronic stroke: psychological wellbeing beyond motor improvement. Int J Rehabil Res 2015;38: 219-225. https://doi.org/10.1097/MRR.0000000000000114
- Calabrò R, Naro A, Russo M, Reitano S, Balletta T, Trombetta G, et al. Do post-stroke patients benefit from robotic verticalization? A pilot-study focusing on a novel neurophysiological approach. Restor Neurol Neurosci 2015; 33: 671-681. https://doi.org/10.3233/RNN-140475
- Castelli L, Iacovelli C, Loreti C, Malizia AM, Barone Ricciardelli I, Tomaino A, et al. Robotic-assisted rehabilitation for balance in stroke patients (ROAR-S): effects of cognitive, motor and functional outcomes. Eur Rev Med Pharmacol Sci 2023; 27: 8198-8211.
- Chen YW, Li KY, Lin CH, Hung PH, Lai HT, Wu CY. The effect of sequential combination of mirror therapy and robot-assisted therapy on motor function, daily function, and self-efficacy after stroke. Sci Rep 2023; 13: 16841. https://doi.org/10.1038/s41598-023-43981-3
- Chen S, Kang J, Peng C, Hsu C, Lin Y, Lai C. Adjustable parameters and the effectiveness of adjunct robotassisted gait training in individuals with chronic stroke. Int J Environ Res Public Health 2022; 19. https://doi.org/10.3390/ijerph19138186
- Chien A, Chang F, Meng N, Yang P, Huang C, Chou L. Clinical efficacy of a new robot-assisted gait training system for acute stroke patients. J Med Biol Eng 2021; 41: 99-107. https://doi.org/10.1007/s40846-020-00590-z
- Daunoraviciene K, Adomaviciene A, Grigonyte A, Griškevičius J, Juocevicius A. Effects of robot-assisted training on upper limb functional recovery during the rehabilitation of poststroke patients. Technol Health Care Off J Eur Soc Eng Med 2018; 26: 533-542. https://doi.org/10.3233/THC-182500
- De Luca R, Maresca G, Balletta T, Cannavò A, Leonardi S, Latella D, et al. Does overground robotic gait training improve non-motor outcomes in patients with chronic stroke? Findings from a pilot study. J Clin Neurosci 2020; 81: 240-245. https://doi.org/10.1016/j.jocn.2020.09.070
- Degami A, Taki S, Imura T, Iwamoto Y, Imada N, Tanaka R, et al. Early initiation of exoskeletal robotic gait training improves functional outcomes in the patients with stroke: a retrospective observational study. Eur Neurol 2023; 86: 121-127. https://doi.org/10.1159/000527710
- Dehem S, Gilliaux M, Stoquart G, Detrembleur C, Jacquemin G, Palumboet S, al. Effectiveness of upper-limb robotic-assisted therapy in the early rehabilitation phase after stroke: a single-blind, randomised, controlled trial. Ann Phys Rehabil Med 2019; 62: 313-320. https://doi.org/10.1016/j.rehab.2019.04.002
- Dundar U, Toktas H, Solak O, Ulasli A, Eroglu S. A comparative study of conventional physiotherapy versus robotic training combined with physiotherapy in patients with stroke. Top Stroke Rehabil 2014; 21: 453-461. https://doi.org/10.1310/tsr2106-453
- Elmas Bodur B, Erdoğanoğlu Y, Asena Sel S. Effects of robotic-assisted gait training on physical capacity, and quality of life among chronic stroke patients: a randomized controlled study. J Clin Neurosci Off J Neurosurg Soc Australas 2024; 120: 129-137. https://doi.org/10.1016/j.jocn.2024.01.010
- Fasoli S, Adans-Dester C. A paradigm shift: rehabilitation robotics, cognitive skills training, and function after stroke. Front Neurol 2019; 10. https://doi.org/10.3389/fneur.2019.01088
- Fundarò C, Giardini A, Maestri R, Traversoni S, Bartolo M, Casale R. Motor and psychosocial impact of robot-assisted gait training in a real-world rehabilitation setting: a pilot study. PLoS One 2018; 13. https://doi.org/10.1371/journal.pone.0191894
- Gueye T, Dedkova M, Rogalewicz V, Grunerova-Lippertova M, Angerova Y. Early post-stroke rehabilitation for upper limb motor function using virtual reality and exoskeleton: equally efficient in older patients. Neurol Neurochir Pol 2021; 55: 91-96. https://doi.org/10.5603/PJNNS.a2020.0096
- Ha Y, Park M. Effects of stroke rehabilitation using gait robot-assisted training and person-centered goal setting: a single blinded pilot study. Healthc Basel Switz 2023; 11. https://doi.org/10.3390/healthcare11040588
- Haolin T, Yuanbin Y, Hu Z, Wenjing Z, Jing Z, Jingfeng T, et al. Efficacy of Daoyin combined with lower limb robot as a comprehensive rehabilitation intervention for stroke patients: a randomized controlled trial. J Tradit Chin Med Chung Tsa Chih Ying Wen Pan 2024; 44: 530-536.
- Hidler J, Nichols D, Pelliccio M, Brady K, Campbell DD, Kahn JH, et al. Multicenter randomized clinical trial evaluating the effectiveness of the Lokomat in subacute stroke. Neurorehabil Neural Repair 2009; 23: 5-13. https://doi.org/10.1177/1545968308326632
- Hirano S, Saitoh E, Imoto D, Ii T, Tsunoda T, Otaka Y. Effects of robot-assisted gait training using the Welwalk on gait independence for individuals with hemiparetic stroke: an assessor-blinded, multicenter randomized controlled trial. J Neuroengineering Rehabil 2024; 21: 76. https://doi.org/10.1186/s12984-024-01370-5
- Hornby TG, Campbell DD, Kahn JH, Demott T, Moore JL, Roth HR. Enhanced gait-related improvements after therapist versus robotic-assisted locomotor training in subjects with chronic stroke: a randomized controlled study. Stroke 2008;39: 1786-1792. https://doi.org/10.1161/STROKEAHA.107.504779
- House G, Burdea G, Polistico K, Grampurohit N, Roll D, Damiani F, et al. A rehabilitation first tournament between teams of nursing home residents with chronic stroke. GAMES Health J 2016; 5: 75-83. https://doi.org/10.1089/g4h.2015.0072
- House G, Burdea G, Polistico K, Roll D, Kim J, Grampurohit N, et al. Integrative rehabilitation of residents chronic post-stroke in skilled nursing facilities: the design and evaluation of the BrightArm Duo. Disabil Rehabil Assist Technol 2016; 11: 683-694. https://doi.org/10.3109/17483107.2015.1068384
- Hsieh YW, Wu CY, Wang WE, Lin K, Chang K, Chen C, et al. Bilateral robotic priming before task-oriented approach in subacute stroke rehabilitation: a pilot randomized controlled trial. Clin Rehabil 2017; 31: 225-233. https://doi.org/10.1177/0269215516633275
- Hung C, Hsieh Y, Wu C, Lin Y, Lin K, Chen C. The effects of combination of robot-assisted therapy with task-specific or impairment-oriented training on motor function and quality of life in chronic stroke. PM R 2016; 8: 721-729. https://doi.org/10.1016/j.pmrj.2016.01.008
- Inoue S, Otaka Y, Kumagai M, Sugasawa M, Mori N, Kondo K. Effects of Balance Exercise Assist Robot training for patients with hemiparetic stroke: a randomized controlled trial. J Neuroengineering Rehabil 2022; 19: 12. https://doi.org/10.1186/s12984-022-00989-6
- Jeon SY, Ki M, Shin JH. Resistive versus active assisted robotic training for the upper limb after a stroke: a randomized controlled study. Ann Phys Rehabil Med 2024; 67:101789. https://doi.org/10.1016/j.rehab.2023.101789
- Kayabinar E, Özalp M, Koçyigit M, As I, Elbasan B. The effects of robotic and conventional gait training in addition to neurodevelopmental treatment on balance, mobility, and health-related quality of life in patients with stroke. Neurol Sci Neurophysiol 2019; 36: 112-119. https://doi.org/10.5152/NSN.2019.10027
- Kayabinar B, Alemdaroğlu-Gürbüz İ, Yilmaz Ö. The effects of virtual reality augmented robot-assisted gait training on dual-task performance and functional measures in chronic stroke: a randomized controlled single-blind trial. Eur J Phys Rehabil Med 2021; 57: 227-237. https://doi.org/10.23736/S1973-9087.21.06441-8
- Kim G, Won Y, Seo J, Ko M. Effects of newly developed compact robot-aided upper extremity training system (Neuro-X®) in patients with stroke: a pilot study. J Rehabil Med 2018; 50: 607-612. https://doi.org/10.2340/16501977-2361
- Kim J, Ko M, Park J, Lee HJ, Nam KY, Nam Y, et al. Efficacy of electromechanically assisted rehabilitation of upper limb function in post-stroke patients: a randomized controlled study. J Rehabil Med Clin Commun 2021; 4: 1000074. https://doi.org/10.2340/20030711-1000074
- Kim Y, Park C, Yoon B, You J. Bolstering cognitive and locomotor function in post-stroke dementia using human-robotic interactive gait training. J Clin Med 2023; 12. https://doi.org/10.3390/jcm12175661
- Lamberti N, Manfredini F, Lissom L, Lavezzi S, Basaglia N, Straudi S. Beneficial effects of robot-assisted gait training on functional recovery in women after stroke: a cohort study. Med-Lith 2021; 57. https://doi.org/10.3390/medicina57111200
- Leblebicier M, Saracoglu I, Yaman F, Sahin E. Effect of robot-assisted gait training on quality of life and depression in patients with hemiplegia. Ann Clin Anal Med 2021; 12: 108-1092. https://doi.org/10.4328/ACAM.20605
- Lee SH, Park G, Cho DY, Kim HY, Lee J, Kim S, et al. Comparisons between endeffector and exoskeleton rehabilitation robots regarding upper extremity function among chronic stroke patients with moderate-to-severe upper limb impairment. Sci Rep 2020; 10: 1806. https://doi.org/10.1038/s41598-020-58630-2
- Lee K, Park G, Shin J. Differences in dual task performance after robotic upper extremity rehabilitation in hemiplegic stroke patients. Front Neurol 2021; 12. https://doi.org/10.3389/fneur.2021.771185
- Lee YH, Ko LW, Hsu CY, Cheng YY. Therapeutic effects of robotic-exoskeleton-assisted gait rehabilitation and predictive factors of significant improvements in stroke patients: a randomized controlled trial. Bioeng Basel Switz 2023; 10. https://doi.org/10.3390/bioengineering10050585
- Leem M, Kim G, Kim K, Yi T, Moon H. Predictors of functional and motor outcomes following upper limb robotassisted therapy after stroke. Int J Rehabil Res 2019; 42:223-228. https://doi.org/10.1097/MRR.0000000000000349
- Linder SM, Rosenfeldt AB, Bay RC, Sahu K, Wolf SL, Alberts JL. Improving quality of life and depression after stroke through telerehabilitation. Am J Occup Ther Off Publ Am Occup Ther Assoc 2015; 69:6902290020p1-10. https://doi.org/10.5014/ajot.2015.014498
- Louie DR, Mortenson WB, Durocher M, Schneeberg A, Teasell R, Yao J, et al. Efficacy of an exoskeleton-based physical therapy program for nonambulatory patients during subacute stroke rehabilitation: a randomized controlled trial. J Neuroengineering Rehabil 2021; 18: 149. https://doi.org/10.1186/s12984-021-00942-z
- Lyukmanov RK, Aziatskaya GA, Mokienko OA, Varako NA, Kovyazina MS, Suponeva NA, et al. Brain-computer interfaces in poststroke rehabilitation: a clinical neuropsychological study. Neurosci Behav Physiol 2019;49: 1038-1046. https://doi.org/10.1007/s11055-019-00835-8
- Ma HI, Hung PH, Lin SH, Chuang IC, Wu CY. Role of selfefficacy in the predictive relationship of motor ability to functional performance after task-related training in stroke: a secondary analysis of longitudinal data. Arch Phys Med Rehabil 2021; 102: 1588-1594. https://doi.org/10.1016/j.apmr.2021.03.017
- Maggio MG, Naro A, Manuli A, Maresca G, Balletta T, Latella D, et al. Effects of robotic neurorehabilitation on body representation in individuals with stroke: a preliminary study focusing on an EEGbased approach. Brain Topogr 2021; 34: 348-362. https://doi.org/10.1007/s10548-021-00825-5
- Maki Y, Ii T, Yamada M, Tanabe S. Factors affecting the efficiency of walking independence in patients with subacute stroke following robot-assisted gait training with conventional rehabilitation. Int J Rehabil Res 2024; 47: 26-33. https://doi.org/10.1097/MRR.0000000000000609
- Manuli A, Maggio MG, Latella D, Cannavò A, Balletta T, De Luca R, et al. Can robotic gait rehabilitation plus Virtual Reality affect cognitive and behavioural outcomes in patients with chronic stroke? A randomized controlled trial involving three different protocols. J Stroke Cerebrovasc Dis Off J Natl Stroke Assoc 2020; 29: 104994. https://doi.org/10.1016/j.jstrokecerebrovasdis.2020.104994
- Manuli A, Maggio M, Stagnitti M, Aliberti R, Cannavò A, Casella C, et al. Is intensive gait training feasible and effective at old age? A retrospective case-control study on the use of Lokomat Free-D in patients with chronic stroke. J Clin Neurosci 2021; 92:159-164. https://doi.org/10.1016/j.jocn.2021.08.013
- Meng G, Ma X, Chen P, Xu S, Li M, Zhao Y, et al. Effect of early integrated robot-assisted gait training on motor and balance in patients with acute ischemic stroke: a single-blinded randomized controlled trial. Ther Adv Neurol Disord 2022; 15:17562864221123195. https://doi.org/10.1177/17562864221123195
- Milani G, Mantovani L, Baroni A, Lamberti N, Basaglia N, Lavezzi S, et al. Variations in health-related quality of life after stroke: insights from a clinical trial on arm rehabilitation with a long-term follow-up. Adv Rehabil Sci Pract. Published online November 29, 2023:1-9. https://doi.org/10.1177/27536351231214845
- Mustafaoglu R, Erhan B, Yeldan I, Gunduz B, Tarakci E. Does robot-assisted gait training improve mobility, activities of daily living and quality of life in stroke? A singleblinded, randomized controlled trial. Acta Neurol Belg 2020; 120: 335-344. https://doi.org/10.1007/s13760-020-01276-8
- Nijenhuis S, Prange G, Amirabdollahian F, Sale P, Infarinato F, Nasr N, et al. Feasibility study into self-administered training at home using an arm and hand device with motivational gaming environment in chronic stroke. J Neuroengineering Rehabil 2015; 12. https://doi.org/10.1186/s12984-015-0080-y
- Norouzi-Gheidari N, Archambault PS, Monte-Silva K, Kairy D, Sveistrup H, Trivino M, et al. Feasibility and preliminary efficacy of a combined virtual reality, robotics and electrical stimulation intervention in upper extremity stroke rehabilitation. J Neuroengineering Rehabil 2021; 18: 61. https://doi.org/10.1186/s12984-021-00851-1
- Ogino T, Kanata Y, Uegaki R, Yamaguchi T, Morisaki K, Nakano S, et al. Effects of gait exercise assist robot (GEAR) on subjects with chronic stroke: a randomized controlled pilot trial. J Stroke Cerebrovasc Dis Off J Natl Stroke Assoc 2020; 29: 104886. https://doi.org/10.1016/j.jstrokecerebrovasdis.2020.104886
- Page SJ, Hill V, White S. Portable upper extremity robotics is as efficacious as upper extremity rehabilitative therapy: a randomized controlled pilot trial. Clin Rehabil 2013; 27:494-503. https://doi.org/10.1177/0269215512464795
- Park JH, Park G, Kim HY, Lee J, Ham Y, Hwang D, et al. A comparison of the effects and usability of two exoskeletal robots with and without robotic actuation for upper extremity rehabilitation among patients with stroke: a single-blinded randomised controlled pilot study. J Neuroengineering Rehabil 2020; 17: 137. https://doi.org/10.1186/s12984-020-00763-6
- Park C, Oh-Park M, Dohle C, Bialek A, Friel K, Edwards D, et al. Effects of innovative hip-knee-ankle interlimb coordinated robot training on ambulation, cardiopulmonary function, depression, and fall confidence in acute hemiplegia. NeuroRehabilitation 2020; 46: 577-587. https://doi.org/10.3233/NRE-203086
- Quinlan E, Dodakian L, See J, McKenzie A, Le V, Wojnowicz M, et al. Neural function, injury, and stroke subtype predict treatment gains after stroke. Ann Neurol 2015; 77: 132-145. https://doi.org/10.1002/ana.24309
- Ranzani R, Lambercy O, Metzger JC, Califfi A, Regazzi S, Dinacci D, et al. Neurocognitive robot-assisted rehabilitation of hand function: a randomized control trial on motor recovery in subacute stroke. J Neuroengineering Rehabil 2020; 17: 115. https://doi.org/10.1186/s12984-020-00746-7
- Rodgers H, Bosomworth H, Krebs HI, van Wijck F, Howel D, Wilson N, et al. Robot-assisted training compared with an enhanced upper limb therapy programme and with usual care for upper limb functional limitation after stroke: the RATULS three-group RCT. Health Technol Assess Winch Engl 2020; 24: 1-232. https://doi.org/10.3310/hta24540
- Rodríguez-Pérez MP, Sánchez-Herrera-Baeza P, Cano-dela-Cuerda R, Camacho-Montaño LR, Serrada-Tejeda S, Pérez-de-Heredia-Torres M. Effects of intensive vibratory treatment with a robotic system on the recovery of sensation and function in patients with subacute and chronic stroke: a non-randomized clinical trial. J Clin Med 2022;11. https://doi.org/10.3390/jcm11133572
- Siotto M, Germanotta M, Santoro M, Cipollini V, Guardati G, Papadopoulou D, et al. Serotonin levels and cognitive recovery in patients with subacute stroke after rehabilitation treatment. Brain Sci 2021; 11. https://doi.org/10.3390/brainsci11050642
- Stolz R, Nayyar R, Louie J, Bower K, Paul S, Ng L. The effectiveness of a novel cable-driven gait trainer (Robowalk) combined with conventional physiotherapy compared to conventional physiotherapy alone following stroke: a randomised controlled trial. Int J Rehabil Res Int Z Rehabil Rev Int Rech Readaptation 2019; 42: 377-384. https://doi.org/10.1097/MRR.0000000000000375
- Takebayashi T, Takahashi K, Amano S, et al. Robot-assisted training as self-training for upper-limb hemiplegia in chronic stroke: a randomized controlled trial. Stroke 2022;53: 2182-2191. https://doi.org/10.1161/STROKEAHA.121.037260
- Taki S, Imura T, Iwamoto Y, Gosho M, Sakai M, Hashimoto K, et al. Effects of exoskeletal lower limb robot training on the activities of daily living in stroke patients: retrospective pre-post comparison using propensity score matched analysis. J Stroke Cerebrovasc Dis 2020; 29: 105176. https://doi.org/10.1016/j.jstrokecerebrovasdis.2020.105176
- Taki S, Imura T, Mitsutake T, Iwamoto Y, Tanaka R, Imada N, et al. Identifying the characteristics of patients with stroke who have difficulty benefiting from gait training with the hybrid assistive limb: a retrospective cohort study. Front Neurorobot 2024; 18. https://doi.org/10.3389/fnbot.2024.1336812
- Taravati S, Capaci K, Uzumcugil H, Tanigor G. Evaluation of an upper limb robotic rehabilitation program on motor functions, quality of life, cognition, and emotional status in patients with stroke: a randomized controlled study. Neurol Sci Off J Ital Neurol Soc Ital Soc Clin Neurophysiol 2022;43: 1177-1188. https://doi.org/10.1007/s10072-021-05431-8
- Timmermans AAA, Lemmens RJM, Monfrance M, Geers RPJ, Bakx W, Smeets RJEM, et al. Effects of task-oriented robot training on arm function, activity, and quality of life in chronic stroke patients: a randomized controlled trial. J Neuroengineering Rehabil 2014; 11: 45. https://doi.org/10.1186/1743-0003-11-45
- Torrisi M, De Cola MC, Buda A, Carioti L, Scaltrito MV, Bramanti P, et al. Self-efficacy, poststroke depression, and rehabilitation outcomes: is there a correlation? J Stroke Cerebrovasc Dis 2018;27: 3208-3211. https://doi.org/10.1016/j.jstrokecerebrovasdis.2018.07.021
- Torrisi M, Maggio M, De Cola M, Zichittella C, Carmela C, Porcari B, et al. Beyond motor recovery after stroke: the role of hand robotic rehabilitation plus virtual reality in improving cognitive function. J Clin Neurosci 2021; 92: 11-16. https://doi.org/10.1016/j.jocn.2021.07.053
- Uivarosan D, Tit D, Iovan C, Nistor-Cseppento DC, Endres L, Lazar L, et al. Effects of combining modern recovery techniques with neurotrophic medication and standard treatment in stroke patients. Sci Total Environ 2019; 679: 80-87. https://doi.org/10.1016/j.scitotenv.2019.05.070
- van Nunen MPM, Gerrits KHL, Konijnenbelt M, Janssen TWJ, de Haan A. Recovery of walking ability using a robotic device in subacute stroke patients: a randomized controlled study. Disabil Rehabil Assist Technol 2015; 10:141-148. https://doi.org/10.3109/17483107.2013.873489
- Volpe B, Krebs H, Hogan N, Edelstein L, Diels C, Aisen M. A novel approach to stroke rehabilitation: robot-aided sensorimotor stimulation. Neurology 2000; 54:1938-1944. https://doi.org/10.1212/WNL.54.10.1938
- Vostrý M, Fischer S, Cmorej PC, Nesvadba M, Peran D, Šín R. Combined therapy for patients after ischemic stroke as a support of social adaptability. Neuro Endocrinol Lett 2019; 40: 329-332.
- Vostry M, Zilcher L. Combined therapy for patients after ischemic stroke from the point of view of comprehensive rehabilitation. J Educ Cult Soc 2020; 11: 119-125. https://doi.org/10.15503/jecs2020.1.119.125
- Wall A, Borg J, Palmcrantz S. Self-perceived functioning and disability after randomized conventional and electromechanically-assisted gait training in subacute stroke: a 6 months follow-up. NeuroRehabil 2019; 45:501-511. https://doi.org/10.3233/NRE-192929
- Wu M, Landry JM, Kim J, Schmit BD, Yen SC, Macdonald J. Robotic resistance/assistance training improves locomotor function in individuals poststroke: a randomized controlled study. Arch Phys Med Rehabil 2014; 95:799-806. https://doi.org/10.1016/j.apmr.2013.12.021
- Wu C-y, Yang C-l, Chuang L-l, Lin KC, Chen HC, Chenet MD, al. Effect of therapist-based versus robot-assisted bilateral arm training on motor control, functional performance, and quality of life after chronic stroke: a clinical trial. Phys Ther 2012;92: 1006-1016. https://doi.org/10.2522/ptj.20110282
- Xie L, Yoon BH, Park C, You J (Sung) H. Optimal intervention timing for robotic-assisted gait training in hemiplegic stroke. Brain Sci 2022; 12: 1058. https://doi.org/10.3390/brainsci12081058
- Yaksi E, Bahadir E, Yasar M, Alisik T, Kurul R, Demirel A. The effect of robot-assisted gait training frequency on walking, functional recovery, and quality of life in patients with stroke. ACTA Neurol Belg 2023; 123: 583-590. https://doi.org/10.1007/s13760-023-02194-1
- Yildiz A, Ahmed I, Mustafaoglu R, Kesiktas FN. Effects of robot-assisted arm training on respiratory muscle strength, activities of daily living, and quality of life in patients with stroke: a single-blinded randomized controlled trial. Physiother Theory Pract. Published online January 2, 2024: 1-9.
- Zengin-Metli D, Özbudak-Demir S, Eraktaş İ, Binay-Safer V, Ekiz T. Effects of robot assistive upper extremity rehabilitation on motor and cognitive recovery, the quality of life, and activities of daily living in stroke patients. J Back Musculoskelet Rehabil 2018; 31: 1059-1064. https://doi.org/10.3233/BMR-171015
- Zhao C, Ju F, Sun W, Jiang S, Xi X, Wang H, et al. Effects of training with a brain computer interface-controlled robot on rehabilitation outcome in patients with subacute stroke: a randomized controlled trial. Neurol Ther 2022; 11: 679-695. https://doi.org/10.1007/s40120-022-00333-z
- Feigin VL, Owolabi MO, World Stroke Organization-Lancet Neurology Commission Stroke Collaboration Group. Pragmatic solutions to reduce the global burden of stroke: a World Stroke Organization-Lancet Neurology Commission. Lancet Neurol 2023; 22: 1160-1206. https://doi.org/10.1016/S1474-4422(23)00277-6
- Feigin VL, Stark BA, Johnson CO, Roth GA, Bisignano C, Abady GG, et al. Global, regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol 2021; 20:795-820. https://doi.org/10.1016/S1474-4422(21)00252-0
- McCambridge AB, Elkins MR. If we can’t see race and ethnicity in research, how will we see racial inequality? J Physiother 2021; 67: 82-83. https://doi.org/10.1016/j.jphys.2021.02.016
- Lang CE, Lohse KR, Birkenmeier RL. Dose and timing in neurorehabilitation: prescribing motor therapy after stroke. Curr Opin Neurol 2015; 28: 549-555. https://doi.org/10.1097/WCO.0000000000000256
- Donnellan-Fernandez K, Ioakim A, Hordacre B. Revisiting dose and intensity of training: opportunities to enhance recovery following stroke. J Stroke Cerebrovasc Dis 2022; 31: 106789. https://doi.org/10.1016/j.jstrokecerebrovasdis.2022.106789
- Lauenroth A, Ioannidis AE, Teichmann B. Influence of combined physical and cognitive training on cognition: a systematic review. BMC Geriatr 2016; 16: 141. https://doi.org/10.1186/s12877-016-0315-1
- Arya KN, Pandian S, Verma R, Garg RK. Movement therapy induced neural reorganization and motor recovery in stroke: a review. J Bodyw Mov Ther 2011; 15:528-537. https://doi.org/10.1016/j.jbmt.2011.01.023
- Bressi F, Cricenti L, Campagnola B, Bravi M, Miccinilli S, Santacaterina F, et al. Effects of robotic upper limb treatment after stroke on cognitive patterns: a systematic review. NeuroRehabilitation 2022; 51:541-558. https://doi.org/10.3233/NRE-220149
- Yuan F, Klavon E, Liu Z, Lopez RP, Zhao X. A systematic review of robotic rehabilitation for cognitive training. Front Robot AI 2021; 8: 605715. https://doi.org/10.3389/frobt.2021.605715
- Zanatta F, Steca P, Fundarò C, Giardini A, Felicetti G, Panigazzi M, et al. Biopsychosocial effects and experience of use of robotic and virtual reality devices in neuromotor rehabilitation: s study protocol. PLoS One 2023; 18: e0282925. https://doi.org/10.1371/journal.pone.0282925
- Lexell J, Brogårdh C. The use of ICF in the neurorehabilitation process. Brogårdh C, Lexell J, eds. NeuroRehabilitation 2015; 36: 5-9. https://doi.org/10.3233/NRE-141184