SPECIAL REPORT
COMMONALITIES IN REHABILITATION DATA ACROSS DIVERSE HEALTH CONDITIONS: A COMPARISON OF SEVEN LARGE EUROPEAN DATABASES
Carlotte KIEKENS, MD1, Helena BURGER, MD, PhD2,3, Paolo CAPODAGLIO, MD4,5, Maria G. CERAVOLO, MD, PhD6, Esther JANSSEN, PhD7,8,9, Greta JURENAITE, MD10, Calogero MALFITANO, MD11,12, Federico PENNESTRI, PhD1, Ruud SELLES, PhD13,14, Gianluca M. TARTAGLIA, MD, PhD4,15, Stefano NEGRINI, MD, PhD1,4 and the PREPARE Group
From the 1IRCCS Galeazzi – Sant’Ambrogio Hospital, Milan, Italy, 2University Rehabilitation Institute, Ljubljana, Slovenia, 3University of Ljubljana, Faculty of Medicine, Ljubljana, Slovenia, 4Department of Biomedical, Surgical and Dental Sciences, University of Milan, Milan, Italy, 5IRCCS Istituto Auxologico Italiano, Milan, Italy, 6Department of Experimental and Clinical Medicine, Marche Polytechnic University, Ancona, Italy, 7IQ Health, Radboud University Medical Center, Radboud Institute for Health Sciences, Nijmegen, The Netherlands, 8School of Allied Health, HAN University of Applied Sciences, Nijmegen, The Netherlands, 9Department of Orthopaedic Surgery, Viecuri Medisch Centrum, Venlo, the Netherlands, 10ISICO (Italian Scientific Spine Institute), Milan, Italy, 11Department of Biomedical Sciences for Health, University of Milan, Milan, Italy, 12Azienda di Servizi alla Persona Istituti Milanesi Martinitt e Stelline e Pio Albergo Trivulzio, Milan, Italy, 13Department of Rehabilitation Medicine, Erasmus MC, University Medical Center Rotterdam, Rotterdam, The Netherlands, 14Department of Plastic and Reconstructive Surgery, Erasmus MC, University Medical Center Rotterdam, Rotterdam, the Netherlands, and 15Policlinico Hospital, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milan, Italy
Objective: To investigate whether rehabilitation data share common characteristics across different health conditions and care settings within the EU Horizon PREPARE project.
Design: Qualitative content analysis, with a comparative study of existing clinical databases.
Subjects/Patients: Individuals with hand and wrist disorders, idiopathic scoliosis, intermittent claudication, lower limb amputation, Parkinson’s disease or Parkinsonism, hip or knee replacement, and temporomandibular disorders.
Methods: Seven rehabilitation-oriented clinical databases were analysed using the International Classification of Functioning, Disability and Health (ICF) framework. Variables were categorized as outcomes, modifiers, or baseline measurements. Commonalities and differences across data domains were identified through iterative consensus meetings among PREPARE partners.
Results: Substantial heterogeneity was observed in data type and depth. Pain and quality of life were the most commonly reported outcomes, whereas discharge status and participation-related measures were rarely reported. The most prevalent modifiers were pharmacological treatments, orthoses or prostheses, and exercise-based interventions. All databases reported baseline information on diagnosis, anthropometry, and demographics; however, assessments of gait autonomy and daily activities were inconsistently documented.
Conclusion: Despite some overlapping domains, rehabilitation data collection remains fragmented and predominantly focused on biomedical aspects. Greater standardization and systematic inclusion of psychosocial and contextual variables are needed for robust predictive modelling and personalized rehabilitation.
LAY ABSTRACT
Rehabilitation is vital to healthcare, yet data collection remains inconsistent. Although numerous clinical databases exist, little is known about the similarities and differences in rehabilitation data across illnesses and settings. In this study, we analysed 7 European rehabilitation databases to identify what information is typically recorded and what is missing. We found that diagnosis, pain level, and overall well-being are often measured, whereas details on how well a patient can walk, perform self-care, or participate in social life after leaving hospital are often lacking. These gaps make it difficult for healthcare providers to compare results or create the best recovery plans for individuals. By standardizing the information we collect, we can improve decision-making and ensure every patient receives care tailored to their specific needs.
Key words:decision support systems; clinical; precision medicine; predictive learning models; rehabilitation.
Citation: J Rehabil Med 2026; 58: jrm45495. DOI: https://doi.org/10.2340/jrm.v58.45495.
Copyright: © 2026 The Author(s). Published by MJS Publishing, on behalf of the Foundation for Rehabilitation Information. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/).
Submitted: Feb 9, 2026; Accepted after revision: Feb 17, 2026; Published: Mar 23, 2026.
Correspondence address: Calogero Malfitano, Department of Biomedical Sciences for Health, University of Milan, Via Luigi Mangiagalli, 31, IT-20133 Milan, Italy. E-mail: calogero.malfitano@unimi.it
Competing interests and funding: SN owns stock in ISICO. The other authors certify that they have no conflict of interest with any financial organization regarding the material discussed in the manuscript.
Funded by the European Union. Views and opinions expressed are, however, those of the authors only and do not necessarily reflect those of the European Union or European Health and Digital Executive Agency (HADEA). Neither the European Union nor the granting authority can be held responsible for them. Grant Agreement 101080288 PREPARE HORIZONHLTH-2022-TOOL-12-01. The work of CK, PC and SN was supported and funded by the Italian Ministry of Health - Ricerca Corrente.
Rehabilitation plays a crucial role in optimizing health outcomes and promoting the well-being of populations. According to the World Health Organization (WHO), approximately 2.6 billion individuals could benefit from rehabilitation services. This need is expected to rise due to ageing populations and an increase in chronic diseases (1, 2). However, access to rehabilitation remains insufficient and inequitable, especially in low- and middle-income countries, where over 50% of those requiring rehabilitation services do not receive them (3, 4). In a healthcare context, rehabilitation is defined as a “multimodal, person-centred, collaborative process, including interventions targeting a person’s capacity (by addressing body structures, functions, and activities/participation) and/or contextual factors related to performance with the goal of optimizing the functioning of persons with health conditions currently experiencing disability or likely to experience disability, or persons with disability” (5). In numerous health conditions, rehabilitation should be considered either at or immediately after the acute onset, and it continues over time in the post-acute and eventually chronic phases (6). Rehabilitation is cross-sectional to many medical fields and shares commonalities between these fields (7). Nevertheless, scarce attention has been given to checking how specific commonalities are implemented in different fields. The EU Horizon PREPARE (Personalised REhabilitation via Novel AI PAtient StRatification StratEgies) project, a European initiative aimed at developing, validating, and implementing robust, clinically relevant, and data-driven computational prediction and stratification tools for the whole field of rehabilitation, offers an important opportunity to evaluate the field cross-sectionally (8). PREPARE focuses on the complexity of rehabilitation, stemming from factors such as multiple health conditions, varied patient experiences, and socioenvironmental contexts (5). The following issues, particular to rehabilitation, are taken into account: (a) functioning, the primary rehabilitation outcome and third health indicator (alongside morbidity and mortality), is multifaceted and mostly individually defined (9); (b) rehabilitation treatment is often complex as it requires more than 1 intervention at a time and a multiprofessional and interdisciplinary approach; (c) people in need of rehabilitation are often multimorbid and require shared decision-making to achieve personalized goals; (d) treatments cross over different healthcare phases; (e) outcomes are not only influenced by clinical indicators but also depend on socioeconomic, behavioural, and living condition indicators and availability of services. For many rehabilitation patients, the most effective treatment approach is multimodal, combining various therapeutic methods to address biological, psychological, and social factors in a coordinated and supportive manner.
In PREPARE, the development of prediction and stratification models is based on large datasets from 7 rehabilitation services in 3 European countries, spanning multiple health conditions, out of a total of 9 pilot cases. These databases were selected after a call shared with the national delegates of the European Society of Physical and Rehabilitation Medicine, for large rehabilitation databases in their countries. The first step of PREPARE was to analyse the commonalities and differences of the variables included in these databases, providing an overview of routinely collected clinical rehabilitation data. These variables demonstrate the attention paid to different topics in rehabilitation patients with varying health conditions. This paper aims to report the PREPARE findings, providing a first answer to the research question: Are there similarities in routine clinical rehabilitation variables collected from patients with different health conditions?
METHODS
Study design
We conducted a qualitative study to compare datasets and rehabilitation processes across 7 European clinical databases. We gradually defined and progressively modified the methodology as needed through a series of consensus meetings every 15 days, where results were presented incrementally. The meetings systematically involved all paper authors, who represented the 7 clinical partners involved, as well as other PREPARE partners, including social scientists, engineers, lawyers, communication specialists, and administrators. Tools were developed and iteratively refined through pilot implementations, feedback from partners, and discussions during general assemblies. Final data validation involved interviews with clinical partners.
Pilot case descriptions
Of a total of 9 pilot cases considered in PREPARE, 2 (people with hypertension and people operated on for spine disorders) were not focused directly on rehabilitation and were excluded from this analysis. The 7 included pilot cases focus on a specific health condition, a particular population and setting, and a rehabilitation process that differs from the others.
The health conditions included, and the reasons for the rehabilitation approach, are:
People with hand and wrist disorders: this database contains a diverse set of common and rare hand and wrist disorders in adult patients collected in collaboration with Xpert Clinics in the Netherlands (10). Common pathologies include osteoarthritis in 1 or multiple joints, neuropathies such as carpal and cubital tunnel syndrome, Dupuytren’s disease, and wrist pathologies, including triangular fibrocartilage complex injuries. The database contains pre-treatment and post-treatment data of patients under either rehabilitation or surgical treatment. The most common treatment goals include pain reduction and (hand) function improvement during daily life (11).
Children with idiopathic scoliosis: idiopathic scoliosis is a deformity of the spine and trunk of unknown aetiology (12); during growth, rehabilitation aims to avoid progression that could cause health issues in adulthood, and specifically pain, plus mental health issues linked to the trunk deformity and progression, possibly leading to camptocormia with related problems in the elderly (13).
People with intermittent claudication: peripheral arterial disease (PAD) is a chronic disease mainly caused by atherosclerosis. Intermittent claudication (IC) is the most common symptom of PAD (14). IC is associated with limited walking distance and poor health-related quality of life. The primary objective of rehabilitation in patients with intermittent claudication entails addressing their specific needs, focusing on enhancing functional (walking) capacity, improving their ability to perform activities, and improving participation (15, 16). Concurrently, effective management also targets modifying risk factors associated with atherosclerosis.
People with lower limb loss: lower limb loss is a change in body structure comprising partial or complete amputation of 1 or both legs, below, through, or above the knee, caused primarily by vascular disease and diabetes, followed by trauma, cancer, and infection (17). It impacts all levels of people’s functioning (body functions, activities, and participation), in relation to personal factors (18). With a prosthesis, which is an environmental factor, many people can walk again and improve their overall health and functioning.
People with Parkinson’s disease or Parkinsonism: Parkinson’s disease and Parkinsonism constitute the second most prevalent neurodegenerative disorders worldwide. They impair independence in activities of daily living, restrict social participation, and diminish quality of life through a broad spectrum of motor symptoms (including bradykinesia, tremor, rigidity, dysarthria, dysphagia, gait disturbances, postural instability, and trunk abnormalities) (19), as well as non-motor symptoms (such as cognitive and mood disorders, psychosis, autonomic dysfunction including bladder and bowel disturbances, orthostatic hypotension, hyposmia, and pain) (20).
People who underwent total hip or knee replacement for primary or secondary osteoarthritis: primary osteoarthritis is a degenerative joint process caused by multiple biological and environmental factors (e.g., genetics, age, overweight, profession, natural wear and tear over time), leading to progressive levels of pain-related disability that cause, in turn, a downward spiral of muscle weakness, functional decline, and psychosocial health worsening; secondary osteoarthritis is still characterized by damage at the joint, but as a consequence of traumatic events and injuries (21); the latest stage of osteoarthritis is usually treated with joint replacement surgery, if the patient is eligible and willing to undergo major surgery; after surgery, global and segmental functional rehabilitation is needed (22, 23).
People with temporomandibular disorders: temporomandibular disorder (TMD) is a complex condition causing pain in the face, head, or neck, often involving the temporomandibular joint and masticatory muscles. Symptoms include joint pain, limited mouth opening, and clicking sounds, with the diagnosis sometimes remaining unclear despite clinical evaluation (24). Effective rehabilitation requires a comprehensive, individualized approach. Management typically involves multimodal therapy, including physical therapy, medication, occlusal splints, and behavioural strategies. Patient education and self-management, including stress reduction and jaw exercises, play a crucial role in promoting long-term recovery. Continuous monitoring and follow-up, aided by data collection tools, help track progress, adjust treatment, and prevent recurrence.
Table I lists the clinical partners of PREPARE and summarizes the main characteristics of their pilot cases.
Included databases
Distinct databases support each rehabilitation case. The main characteristics of each database are reported in Table II. Below, we describe each of them in more detail.
Hand and wrist disorders: The “Pulse” database has been operating in the Netherlands since 2011, aiming to enhance clinical care by providing feedback to clinicians on treatment outcomes and patient experiences and facilitating research. The content of the database has evolved. Initially, it included patient-reported outcomes and clinician-reported metrics such as grip strength and range of motion. Psychological questionnaires were integrated in 2017 to further personalize patient care. Subsequently, this database expanded to include preoperative screening tools and clinician dashboards.
Idiopathic scoliosis in children: The ScoliosisManager database, developed by ISICO in Italy in 2003, encapsulated all spinal deformity rehabilitation operations and research operations. The platform allows real-time data updates by healthcare providers and offers comprehensive modules for physicians (e.g., patient assessment, diagnosis, prescription management, X-ray data, storage of images and documents, brace sensor analysis, clinical questionnaires, and a clinical diary) and physical therapists (e.g., focuses on patient assessment, creating active self-correction movements, and formulating exercise plans). A mobile application introduced in 2016 has improved patient engagement by providing personalized feedback and educational content.
Intermittent claudication: The Chronic CareNet Quality system, established in 2015, collects data from primary care physiotherapy practices in the Netherlands. Variables included in the database were patient characteristics (e.g., age, sex, body mass index), treatment processes (e.g., treatment duration, number of treatment sessions, achievement of treatment goal), and patient-reported outcome measures (quality of life and walking distances). Predictive tools like KomPas facilitate shared decision-making by offering personalized outcome forecasts. The system’s integration with national guidelines ensures standardized treatment across healthcare providers.
Lower limb loss: A dedicated Excel database (Microsoft Corp, Armonk, NY, USA) initiated in 2021 in Slovenia tracks 417 variables across different professional groups, including physical and rehabilitation medicine, internal medicine, nursing, physiotherapy, occupational therapy, psychology, social work, and prosthetics. This database supports multidisciplinary collaboration and aims to identify predictors of rehabilitation outcomes, such as safe prosthetic fitting, and increased risk of falling and increased risk of wound development on the residual limb.
Parkinson’s disease: An electronic database developed since 2007 in Italy using Claris FileMaker® Pro records follow-up data for patients with Parkinson’s disease or Parkinsonism. During each visit, data were recorded on demographics, general health (including BMI and blood pressure values), disease and comorbidities history, medication schedule, functional surgery parameters, type and duration of rehabilitation treatment, complications, drug side effects, and standard assessments of disease severity (motor and cognitive). The database facilitates longitudinal tracking of disease progression and treatment efficacy, enabling the identification of key prognostic factors.
Hip and knee replacement: A patient-centred database for osteoarthritic patients undergoing inpatient rehabilitation after total hip or knee replacement was manually set for PREPARE. Preoperative data, surgical ward data, and rehabilitation ward data were linked by the principal investigator and researchers through the hospital patient identifier (MSP Trakcare). In this way, the entire inpatient pathway could be recomposed in search of potentially predictive factors, including pre-admission and post-discharge information already collected in the medical records (e.g., pre-existing comorbidities, pre-existing pharmacological treatment, demographic information, working status, living place, estimated hours of care needed after discharge, presence of a caregiver at home, potential frailty of the caregiver him/herself). Seventy-three variables were considered for each patient.
Temporomandibular disorders: A database developed in Italy in 2023–2024 includes diagnostic criteria, screening methods, and treatment protocols for TMD, with real-time data entry by clinicians. This database aims to improve the standardization of care and support research on treatment outcomes. It is mainly based on the diagnostic criteria for TMD, while adding information to address the recognised weaknesses of the Diagnostic Criteria–TMD, such as considering alternative structural or systemic causes and including a broader assessment of the muscles.
Variables categorization
Variables were divided into 3 main categories:
Outcomes: Variables used to verify the results; more specifically, clinical outcomes that are measurable changes in health, symptoms, functioning, or quality of life resulting from the natural history or rehabilitation treatment.
Modifiers: Variables introduced due to treatment, i.e., therapeutic strategies that alter the progression or outcome of the health condition (e.g., exercises, drugs, surgery, or other strategies aimed at managing symptoms, improving functioning, preventing complications, or slowing the progression of the underlying condition). Also, other factors such as lifestyle changes (e.g., smoking cessation) or new comorbidities (e.g., heart disorders or diabetes mellitus) can be considered.
Measurements: Variables collected at baseline, before any treatment, such as demographic characteristics or quantified disease-related or functional data, serve as the basis for assessing potential improvements.
Classifiers
We used the International Classification of Functioning, Disability and Health (ICF) (25) framework to classify the variables and enable comparison across all databases. According to the category of variables considered, it was necessary to either use or add further categorizers. We added patient reported outcome measures (PROMs) and discharge planning as outcome variables, as well as demographics, patient measures, laboratory data, risk factors, and costs for baseline measurements. Finally, for modifiers, we decided to use the following categories: rehabilitation, exercise therapy, orthoses, prostheses, physical modalities, other non-pharmacological and non-surgical interventions, drugs, surgery, prevention, medical history, and treatment timing.
Data availability
All data supporting the findings of this study are included in the presentation. Additional details can be obtained from the corresponding author upon reasonable request.
RESULTS
Fig. 1 reports the outcomes of the PREPARE databases. The social, behavioral and psychological indicators are reported in italics in this and the following figures. The databases included a median of 4 (range 2–5) of the 6 categories, with no database covering all categories. The most common categories were PROMs and impairments, included in 6 databases. Five databases contained data on some activities, but with differences in the types of activities considered. For participation, only the return-to-work component was included (3 databases). A median of 9 variables (range 6–12) was included. The most frequently measured variables were pain and quality of life (6 databases), followed by body structures and satisfaction (5 databases). We did not find any variables shared across all databases.
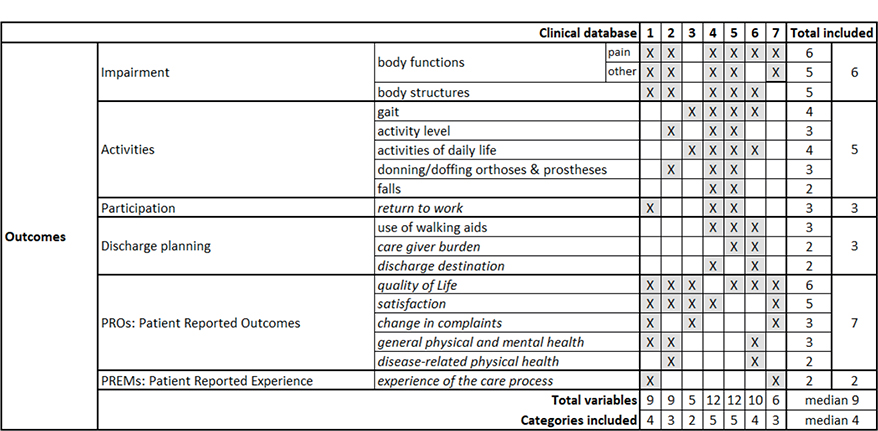
Fig. 1. Outcome categories included in the considered databases. 1. Erasmus MC, Universitair Medisch Centrum, Rotterdam, the Netherlands; 2. ISICO (Istituto Scientifico Italiano Colonna Vertebrale), Milan, Italy; 3. Radboud Universitair Medisch Centrum, Nijmegen, the Netherlands; 4. Univerzitetni Rehabilitacijski Institut Republike Slovenije-Soca, Liubljana, Slovenia; 5. Università Politecnica delle Marche, Ancona, Italy; 6. IRCCS Ospedale Galeazzi Sant’Ambrogio, Milan, Italy; 7. Università degli Studi di Milano, Milan, Italy.
Fig. 2 shows the modifiers. The databases included a median of 7 modifiers (range 4–12) and considered 4 (2–5) of the 8 categories, with none considering all categories. The modifiers encompass various rehabilitation approaches, exhibiting notable variability. While all databases include rehabilitation or exercise approaches, the 2 most reported treatments are complex multimodal rehabilitation and exercises, each documented in 4 databases. The most frequently mentioned modifiers (present in 5 databases) are orthoses and prostheses and oral drugs, with variable therapy duration reported in 4 cases. All other variables appear in 3 or fewer databases.
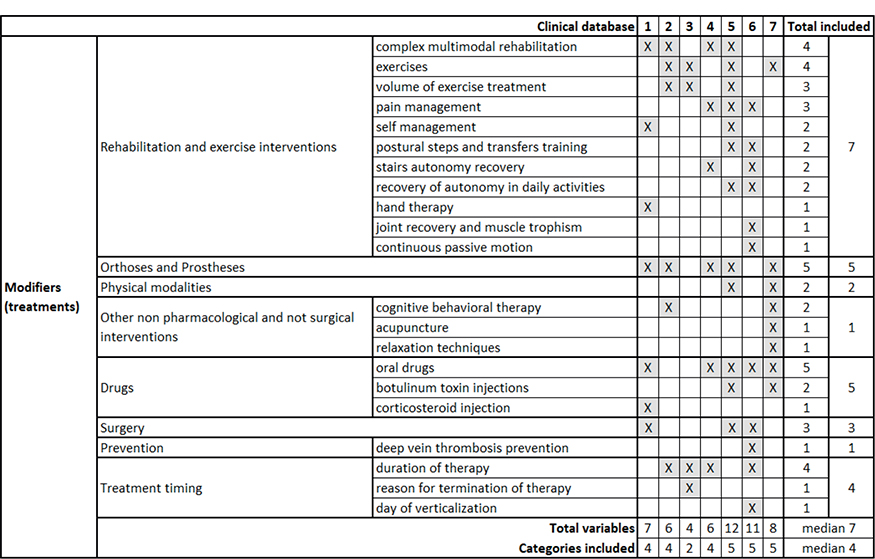
Fig. 2. Modifiers (treatments) included in the considered databases. 1. Erasmus MC, Universitair Medisch Centrum, Rotterdam, the Netherlands; 2. ISICO (Istituto Scientifico Italiano Colonna Vertebrale), Milan, Italy; 3. Radboud Universitair Medisch Centrum, Nijmegen, the Netherlands; 4. Univerzitetni Rehabilitacijski Institut Republike Slovenije-Soca, Liubljana, Slovenia; 5. Università Politecnica delle Marche, Ancona, Italy; 6. IRCCS Ospedale Galeazzi Sant’Ambrogio, Milan, Italy; 7. Università degli Studi di Milano, Milan, Italy.
Fig. 3 shows the measurements, mainly the variables at baseline assessment and all variables that are neither outcomes nor modifiers. The databases included a median of 14 measurements (range 9–18) and considered 7 (5–9) of the 10 categories, with no database including all of them. Among the categories, disease diagnosis, demographics (age and sex), and body structures (BMI) were included in all databases. PROMs were present at baseline in 6 of 7 databases; the duration of disease, comorbidities, and risk factors were included in 5 databases. Other measurements appeared in 4 or fewer cases.

Fig. 3. Baseline measurements included in the considered databases. 1. Erasmus MC, Universitair Medisch Centrum, Rotterdam, the Netherlands; 2. ISICO (Istituto Scientifico Italiano Colonna Vertebrale), Milan, Italy; 3. Radboud Universitair Medisch Centrum, Nijmegen, the Netherlands; 4. Univerzitetni Rehabilitacijski Institut Republike Slovenije-Soca, Liubljana, Slovenia; 5. Università Politecnica delle Marche, Ancona, Italy; 6. IRCCS Ospedale Galeazzi Sant’Ambrogio, Milan, Italy; 7. Università degli Studi di Milano, Milan, Italy.
Overall, we found 17 social, behavioral, and psychological indicators: quality of life, return to work, caregiver burden, discharge destination, satisfaction, change in complaints, general physical and mental health, disease-related physical health, experience of the care process, type of work, PROMs, education, age, sex, ethnicity, smoking. The least frequently reported information in the databases is caregiver burden and general physical and mental health (2 out of 7).
DISCUSSION
The question we aimed to address in this paper was: Are there commonalities in the real-world collected data on rehabilitation for patients with various health conditions? Overall, we clearly see a trend of including similar categories across all databases. However, the most common categories remain those related to anthropometric, disease-specific, and impairment information. The “classical” biomedical approach appears to be more established (and includes more validated variables) than the biopsychosocial approach, at least in the databases considered. High importance is placed on patient-specific measures, both as outcomes and as baseline assessments. In contrast, core functioning data regarding activities and participation are less frequently considered. While similarities are evident, progress still needs to be made before achieving a truly standardized approach to data collection in rehabilitation across different health conditions.
Rehabilitation treatment is often complex and multimodal, involving multiple interventions simultaneously and an interdisciplinary multiprofessional approach (5). The 7 different databases analysed in this paper represent a significant portion of the rehabilitation field, even if musculoskeletal conditions are predominant. They differed significantly in the quantity and types of indicators collected, providing a broad view of the available outcomes, measurements, and therapy modifiers within rehabilitation. The findings highlight the variability in rehabilitation practices across various conditions, reflecting patients’ diverse needs and emphasizing the multimodal approach used. Our comparative analysis of 7 pilot cases representing the rehabilitation field revealed both common and unique features. Shared aspects include standardized data collection, validated outcome measures, and the inclusion of patient-reported outcomes. Variations were observed in the types of variables gathered, data entry methods, software programs used, and the extent to which databases are integrated into clinical practice. Additionally, the level of technological integration varied, with only some databases offering real-time dashboards and mobile applications that enhance clinician–patient interaction.
ICF is the common framework for rehabilitation (25). The use of the ICF as standardized common terminology has enabled meaningful comparisons between different cases. However, while the ICF served its purpose, it was unable to fully describe the included variables. In the era of big data, developing common vocabularies and data structures for clinical database development could be vital not only to better describe (and improve through research) clinical practices but also to allow for that database information to be combined for joint analysis. For example, while the ICF is a framework for common terminology, the same concepts defined by the same ICF terminology may still be coded differently in each database. Moreover, the ICF fails to provide terms for low-level concepts in rehabilitation at the level of the measurements or treatments (26), and does not define relationships between concepts. Initiatives like the multiprofessional Observational Health Data Sciences and Informatics (OHDSI) international community (27), promoted by PREPARE within the field of rehabilitation (8), could be instrumental in this regard. OHDSI adopted the Observational Medical Outcomes Partnership (OMOP) common data model (CDM) as a platform for standardizing the structure, content, and analytics of medical data. The OMOP-CDM is an open community data standard that enables efficient analyses to produce reliable evidence (28). A standardized framework to generate and evaluate patient-level prediction models using observational healthcare data has also been developed (29). It has been implemented as open-source software utilizing the OMOP-CDM to facilitate the sharing of models and the reproducibility of model evaluations across multiple observational datasets. A central component of the OMOP CDM is the OHDSI standardized vocabularies. The OMOP-CDM allows for standardized representation of the same data. Representing the same data across databases enables multicentre studies to be performed with standardized analytics that leverage the knowledge base within characterization, population-level effect estimation, and patient-level prediction studies.
While OMOP-CDM has been developed over many years and contains millions of medical concepts, we noticed that many typical rehabilitation concepts are still lacking in the current OHDSI vocabularies. Moreover, there is currently a limited possibility for structuring PROMs, PREMs, and complex longitudinal treatments in the existing OMOP-CDM domains. Therefore, some PREPARE partners joined forces to establish an OHDSI – Rehabilitation Workgroup (30). Such initiatives could encourage the inclusion of factors influencing the availability and utilization of effective care – such as patients’ income, insurance, culture, health literacy, as well as external factors related to healthcare providers (e.g., knowledge and beliefs), the healthcare system (e.g., staffing, wait times, incentives), and communities (e.g., rurality, transportation options, social supports). By promoting a standardized approach to data collection and analysis, the PREPARE project has the potential to transform rehabilitation practices across Europe and beyond.
The included databases reflect essential parts of the daily clinical practice of the partners involved. They were mainly developed to treat patients while collecting information for research purposes. To ensure real-world routine clinical data collection, decisions have been made to minimize the burden on physicians and gather useful information. As the primary focus is clinical, these databases were not designed to be “comprehensive” but to be “purpose-oriented”. Additionally, some of them were created many years ago and have gradually evolved into their current form, expanding data collection while keeping the workload manageable. This is a key characteristic of our study: not a depiction of what should be done, but of what is typically done.
Another important element to note is that the databases we explored are limited in number and do not allow for subgrouping. Nevertheless, they cover the entire field and represent a large number of patients across various areas of rehabilitation: inpatients, outpatients, rehabilitation and habilitation, acute, post-acute and chronic care, children, adults, and the elderly. It is worth noting that these databases are pioneers in rehabilitation, where the biopsychosocial approach makes data collection difficult. The limited number of databases could have contributed to the variability observed and, hypothetically, it is possible that within a specific area there could be more consistency in the rehabilitation of different health conditions. Nonetheless, this remains a hypothesis. In this regard, guiding health information systems to collect data for rehabilitation through routine health facility reporting built around a standard set of indicators (31) would provide a comprehensive view of the available outcomes, measurements, and therapy modifiers representative of the whole rehabilitation field and enhance the definition of rehabilitation sector targets, outcomes, and clinical decision-making across different health conditions.
Strengths and limitations
This paper has several strengths and weaknesses. Strengths include the holistic approach to rehabilitation across various health conditions; international and multidisciplinary collaboration among 7 diverse groups; the use of the ICF framework for structured comparison; the inclusion of large, existing databases; the comprehensive qualitative process used to develop the report; and the representation of real-world clinical practice through variables applicable in everyday patient care. The weaknesses include the limited external validity of findings due to the small number of analysed databases and their heterogeneity, the underrepresentation of psychosocial and contextual factors, and a lack of advanced quantitative analyses. Additionally, some databases are recent or incomplete, which can affect the comprehensiveness of the data.
Conclusion
This study demonstrates that rehabilitation databases across diverse health conditions share certain categories of information but remain heterogeneous and predominantly biomedical in focus. Psychosocial, contextual, and participation-related data are underrepresented, limiting a comprehensive understanding of the biopsychosocial nature of rehabilitation. Standardizing and expanding data collection will be essential to build robust, interoperable databases that can support personalized care and predictive modelling. Future efforts should prioritize increasing database inclusion, enhancing data standardization, and adopting rigorous statistical methods to refine personalized rehabilitation models and better capture the biopsychosocial complexity of patient care.
ACKNOWLEDGEMENTS
Contributors: PREPARE Group members: Emin Aghayev; Vasilis Alepopoulos; Giuseppe Banfi; Marianna Capecci; Irene Ferrario; Charalampos Georgiadis; Georgios Giannios; Margarita Gramatikopoulou; Christian Herrmann; Lisa Hoogendam; Thomas Hoogeboom; Shahnawaz Khijmatgar; Ioannis Kompatsiaris; Vasilios Kotsis; Lampros Mpaltadoros; Spiros Nikolopoulos; Erik Novak; George R. Patias; Petros Patias; Arianna Poli; Themistocles Roustanis; Dimitrios Tsaopoulos; Haris Zaharatos.
Ethical clearance: This paper does not analyse individual patient data, but only the number and type of variables collected across databases; therefore, no ethical approval was required.
REFERENCES
- Institute for Health Metrics and Evaluation. WHO Rehabilitation Need Estimator [Serial on the Internet]. 2024 [cited 2025 Aug 30]. Available from: vizhub.healthdata.org/rehabilitation
- World Health Organization. Rehabilitation [Fact sheet] [Serial on the Internet]. 2024 [cited 2025 Aug 30]. Available from: www.who.int/news-room/fact-sheets/detail/rehabilitation
- Cieza A, Causey K, Kamenov K, Hanson SW, Chatterji S, Vos T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 2021; 396: 2006–2017. https://doi.org/10.1016/S0140-6736(20)32340-0
- World Health Organization. Strengthening rehabilitation in health systems [Serial on the Internet]. Geneva; 2023 [cited 2025 May 5]. Available from: https://apps.who.int/gb/ebwha/pdf_files/WHA76/A76_R6-en.pdf
- Negrini S, Selb M, Kiekens C, Todhunter-Brown A, Arienti C, Stucki G, et al. Rehabilitation definition for research purposes: a global stakeholders’ initiative by Cochrane Rehabilitation. Eur J Phys Rehabil Med 2022; 58: 333–341. https://doi.org/10.23736/S1973-9087.22.07509-8
- European Physical and Rehabilitation Medicine Bodies Alliance. White Book on Physical and Rehabilitation Medicine (PRM) in Europe. Chapter 8. The PRM specialty in the healthcare system and society. Eur J Phys Rehabil Med 2018; 54: 261–278. https://doi.org/10.23736/S1973-9087.18.05152-3
- European Physical and Rehabilitation Medicine Bodies Alliance. White Book on Physical and Rehabilitation Medicine (PRM) in Europe. Chapter 7. The clinical field of competence: PRM in practice. Eur J Phys Rehabil Med 2018; 54: 230–260. https://doi.org/10.23736/S1973-9087.18.05151-1
- PREPARE Consortium. PREPARE – Personalised Rehabilitation via Novel AI Patient Stratification Strategies [Serial on the Internet]. 2025 [cited 2025 Aug 30]. Available from: https://prepare-rehab.eu/
- Stucki G, Bickenbach J. Functioning: the third health indicator in the health system and the key indicator for rehabilitation. Eur J Phys Rehabil Med 2017; 53. https://doi.org/10.23736/S1973-9087.17.04565-80
- Selles RW, Wouters RM, Poelstra R, van der Oest MJW, Porsius JT, Hovius SER, et al. Routine health outcome measurement: development, design, and implementation of the Hand and Wrist Cohort. Plast Reconstr Surg 2020; 146: 343–354. https://doi.org/10.1097/PRS.0000000000007008
- Shoda Y, Mischel W, Wright JC. The role of situational demands and cognitive competencies in behavior organization and personality coherence. J Pers Soc Psychol 1993; 65: 1023–1035. https://doi.org/10.1037//0022-3514.65.5.1023
- Negrini S, Donzelli S, Aulisa AG, Czaprowski D, Schreiber S, de Mauroy JC, et al. 2016 SOSORT guidelines: orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis Spinal Disord 2018; 13: 3. https://doi.org/10.1186/s13013-017-0145-8
- Negrini S, Hresko TM, O’Brien JP, Price N, SOSORT Boards, SRS Non-Operative Committee. Recommendations for research studies on treatment of idiopathic scoliosis: consensus 2014 between SOSORT and SRS non-operative management committee. Scoliosis 2015; 10: 8. https://doi.org/10.1186/s13013-014-0025-4
- Fowkes FGR, Rudan D, Rudan I, Aboyans V, Denenberg JO, McDermott MM, et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet 2013; 382: 1329–1340. https://doi.org/10.1016/S0140-6736(13)61249-0
- Gerhard-Herman MD, Gornik HL, Barrett C, Barshes NR, Corriere MA, Drachman DE, et al. 2016 AHA/ACC Guideline on the management of patients with lower extremity peripheral artery disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2017; 69: 1465–1508. https://doi.org/10.1016/j.jacc.2016.11.008
- Aboyans V, Ricco J-B, Bartelink M-LEL, Björck M, Brodmann M, Cohnert T, et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS). Eur Heart J 2018; 39: 763–816. https://doi.org/10.1093/eurheartj/ehx095
- Narres M, Kvitkina T, Claessen H, Droste S, Schuster B, Morbach S, et al. Incidence of lower extremity amputations in the diabetic compared with the non-diabetic population: a systematic review. PLoS One 2017; 12: e0182081. https://doi.org/10.1371/journal.pone.0182081
- Hunter SW, Batchelor F, Hill KD, Hill A, Mackintosh S, Payne M. Risk factors for falls in people with a lower limb amputation: a systematic review. PM&R 2017; 9: 170. https://doi.org/10.1016/j.pmrj.2016.07.531
- Capecci M, Baldini N, Campignoli F, Lombardo LP, Andrenelli E, Ceravolo MG. Clinical and functional evolution in subjects with Parkinson’s disease during SARS-CoV-2 pandemic. Appl Sc (Basel) 2023; 13. https://doi.org/10.3390/app13021126
- Poewe W. Non–motor symptoms in Parkinson’s disease. Eur J Neurol 2008; 15: 14–20. https://doi.org/10.1111/j.1468-1331.2008.02056.x
- Hurley M, Dickson K, Hallett R, Grant R, Hauari H, Walsh N, et al. Exercise interventions and patient beliefs for people with hip, knee or hip and knee osteoarthritis: a mixed methods review. Cochrane Database Syst Rev 2018; 4: CD010842. https://doi.org/10.1002/14651858.CD010842.pub2
- Artz N, Elvers KT, Lowe CM, Sackley C, Jepson P, Beswick AD. Effectiveness of physiotherapy exercise following total knee replacement: systematic review and meta-analysis. BMC Musculoskelet Disord 2015; 16: 15. https://doi.org/10.1186/s12891-015-0469-6
- Minns Lowe CJ, Davies L, Sackley CM, Barker KL. Effectiveness of land-based physiotherapy exercise following hospital discharge following hip arthroplasty for osteoarthritis: an updated systematic review. Physiotherapy 2015; 101: 252–265. https://doi.org/10.1016/j.physio.2014.12.003
- Tartaglia GM, Lodetti G, Paiva G, De Felicio CM, Sforza C. Surface electromyographic assessment of patients with long lasting temporomandibular joint disorder pain. J Electromyogr Kinesiol 2011; 21: 659–664. https://doi.org/10.1016/j.jelekin.2011.03.003
- World Health Organization. International Classification of Functioning, Disability and Health (ICF) [Serial on the Internet]. Endorsed by the 54th World Health Assembly on 22 May 2001 (Resolution WHA 54.21). 2001 [cited 2025 Aug 30]. Available from: www.who.int/standards/classifications/international-classification-of-functioning-disability-and-health
- Janssen ERC, Punt IM, van Soest J, Heerkens YF, Stallinga HA, ten Napel H, et al. Operationalizing and digitizing person-centered daily functioning: a case for functionomics. BMC Med Inform Decis Mak 2024; 24: 184. https://doi.org/10.1186/s12911-024-02584-2
- Observational Health Data Sciences and Informatics (OHDSI). OHDSI: Observational Health Data Sciences and Informatics [Serial on the Internet]. 2025 [cited 2025 Aug 30]. Available from: https://www.ohdsi.org/
- Hripcsak G, Schuemie MJ, Madigan D, Ryan PB, Suchard MA. Drawing reproducible conclusions from observational clinical data with OHDSI. Yearb Med Inform 2021; 30: 283–289. https://doi.org/10.1055/s-0041-1726481
- Reps JM, Schuemie MJ, Suchard MA, Ryan PB, Rijnbeek PR. Design and implementation of a standardized framework to generate and evaluate patient-level prediction models using observational healthcare data. J Am Med Inform Assoc 2018; 25: 969–975. https://doi.org/10.1093/jamia/ocy032
- Esther Janssen, Ruud Selles. OHDSI Workgroup Objectives and Key Results (OKR) Rehabilitation Workgroup [Serial on the Internet]. 2024 [cited 2025 Aug 30]. Available from: www.ohdsi.org/wp-content/uploads/2024/04/Rehabilitation-24.pdf
- World Health Organization. Routine Health Information Systems – Rehabilitation Toolkit [Serial on the Internet]. 2025 [cited 2025 Aug 30]. Available from: www.who.int/tools/routine-health-information-systems---rehabilitation-toolkit