ORIGINAL ARTICLE
WHO MAY BENEFIT FROM ROBOT-ASSISTED GAIT TRAINING WITH AN EXOSKELETON IN SUBACUTE STROKE PATIENTS? A PRESPECIFIED ANALYSIS
Won Hyuk CHANG, MD, PhD1, Tae-Woo KIM, MD2,3, Hyoung Seop KIM, MD, PhD4, Fazah Akhtar HANAPIAH, MBBCH5, Jong Weon LEE, MD6, Seung-Hyeon HAN, OT6, Chai Wen JIA, MD, PhD7, Dae Hyun KIM, MD, PhD1 and Deog Young KIM, MD, PhD6
From the 1Department of Physical and Rehabilitation Medicine, Center for Prevention and Rehabilitation, Heart Vascular and Stroke Institute, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea, 2TBI Rehabilitation Center, National Traffic Injury Rehabilitation Hospital, Gyeonggi-do, Republic of Korea, 3Department of Rehabilitation Medicine, Seoul National University College of Medicine, Seoul, Republic of Korea, 4Department of Rehabilitation Medicine, Pohang Stoke and Spine Hospital, Pohang, Republic of Korea, 5Faculty of Medicine, Universiti Teknologi MARA, Selangor, Malaysia, 6Department and Research Institute of Rehabilitation Medicine, Yonsei University College of Medicine, Seoul, Republic of Korea, and 7Department of Psychology, Faculty of Social Sciences, Raffles University, Johor, Malaysia
Objective: To identify factors associated with the achievement of independent gait after the robot-assisted gait training (RAGT) with an exoskeletal wearable robot in subacute stroke patients.
Design: An international, multicentre, randomized, controlled trial.
Subjects/Patients: This prespecified analysis was performed on 58 and 69 subacute stroke patients in the RAGT and control groups.
Methods: Each RAGT and the conventional gait training was provided 5 times per week for a period of 4 weeks. A Functional Ambulation Categories score of > 3 immediately post-intervention was defined as independent ambulation and clinical significance. Univariate and multivariate binary logistic regression models were used to determine possible predictors of clinically significant response to the RAGT and the conventional gait training.
Results: The 2 independent factors with the greatest impact on the response to RAGT for the achievement of independent gait were initial cognitive function and affected lower extremity power (p < 0.05). However, in the control group, stroke duration from onset to treatment and affected lower extremity power were significant independent factors (p < 0.05).
Conclusion: This prespecified analysis suggests that the efficacy of RAGT with a wearable exoskeleton appears to be less dependent on time since onset within the early subacute phase, highlighting the importance of preserved cognitive function.
LAY ABSTRACT
Stroke survivors often need help learning to walk again. This study compared conventional and an exoskeletal wearable robot-based gait training to see what helps patients walk independently after treatment. We found that having some baseline leg strength was important for both types of therapy. But the other keys to success were quite different. When it comes to conventional gait training, it is really important to start the exercises as soon as possible after the stroke. For patients using an exoskeletal wearable robot, the time since their stroke was less important. Instead, it was their good cognitive function that made them successful. This suggests that using an exoskeletal wearable robot to train their gait could be a great option for stroke survivors to recover, even if it has been a while since their stroke. However, it is important to make sure the patient has the cognitive ability to actively use the technology.
Key words: stroke; ambulation; rehabilitation; robot therapy; robot-assisted gait training; overground gait training.
Citation: J Rehabil Med 2026; 58: jrm45822. DOI: https://doi.org/10.2340/jrm.v58.45822.
Copyright: © 2026 The Author(s). Published by MJS Publishing, on behalf of the Foundation for Rehabilitation Information. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/).
Submitted: Mar 30, 2026; Accepted after revision: Jun 1, 2026; Published: Jun 17, 2026.
Correspondence address: Deog Young Kim, Department of Rehabilitation Medicine and Research Institute of Rehabilitation Medicine, Yonsei University College of Medicine, 50-1 Yonsei-ro, Seodaemun-gu, Seoul 03722, Korea. E-mail: kimdy@yuhs.ac
Competing interests and funding: The authors have no conflicts of interest to declare.
This work was supported by the Korea Medical Device Development Fund grant funded by the Korea government (the Ministry of Science and ICT, the Ministry of Trade, Industry and Energy, the Ministry of Health & Welfare, the Ministry of Food and Drug Safety (Project Number: RS-2021-KD000003).
Robot-assisted gait training (RAGT) has emerged as a pivotal therapeutic intervention in neurorehabilitation since its introduction in the late 1990s, originally having been developed to overcome the labour-intensive limitations of manual partial bodyweight-supported treadmill training. By facilitating high-intensity, repetitive, and task-specific practice with consistent kinematic guidance, RAGT allows for a dosage of training that far exceeds what is typically feasible with conventional physical therapy (1, 2). Extensive research supports its efficacy; notably, a recent review established that a treadmill-based RAGT, in combination with physiotherapy, significantly increases the odds of independent walking recovery, particularly in non-ambulatory patients at the subacute stage (3). Furthermore, clinical trials suggest that the “window of opportunity” for RAGT is optimal within the early subacute period, where heightened neuroplastic potential allows for more effective motor relearning compared with the chronic phase (4).
Despite the clinical utility of treadmill-based RAGT, it has been noted that this approach differs from the conditions of actual ground walking (5) and that it can be difficult to align the robot’s movements with the patient’s muscular contraction efforts or the passive characteristics of the musculoskeletal system (6). Consequently, overground gait training using an exoskeleton has recently been proposed as an alternative form of RAGT. This RAGT has been proposed to promote the activation of the nervous system by inducing active participation from the patient who performed active balance control, weight shift, and muscle activation (6).
Recently, we reported the effect of overground gait training using a torque-assisted exoskeleton in patients with subacute stroke on the recovery of ambulatory function (7). Our previous study revealed that there was no significant difference in improving ambulatory function between overground gait training using a torque-assisted exoskeleton and conventional gait training. Nevertheless, given that both groups exhibited enhancements in ambulatory function, the identification of the factors that contribute to the effectiveness of each type of gait rehabilitation could determine the indications for each approach. Therefore, the aim of the current study was to identify factors associated with the achievement of independent gait after the RAGT with an exoskeletal wearable robot in subacute stroke patients. In this analysis, we investigated the characteristics of patients with subacute stroke for the appropriate indications for an exoskeleton in patients with subacute stroke through this prespecified analysis. The identification of the appropriate indication of RAGT with an exoskeleton will aid in the design of individual treatment plans and the accurate stratification of patients for better outcomes after RAGT in patients with subacute stroke.
METHODS
Study design
This was a prespecified analysis of an international, multicentre, randomized, controlled trial with blinded outcome evaluation in patients with subacute stroke (8). The study was conducted in 4 hospitals in the Republic of Korea and 2 hospitals in Malaysia. The trial was registered at ClinicalTrials.gov (NCT05157347). The protocol (8) was approved by the Institutional Review Board (IRB) of each hospital (IRB of Severance Hospital, South Korea (IRB no. 1-2021-0031), IRB of National Traffic Injury Rehabilitation Hospital (No. NTRH-21016), IRB of Samsung Medical Center (IRB no. 2021-07-021), IRB of the National Health Insurance Service Ilsan Hospital (No. NHIS- 2021-07-029), and IRB of the Universiti Teknologi MARA (No. REC/04/2021 (MR/26)), and conforms to the Declaration of Helsinki. All participants provided written informed consent before starting the study procedures.
Participants were randomly assigned, in a 1:1 ratio, to the RAGT group and the control group. After randomization, each participant attended a total of 20 sessions, 5 times a week, over 4 weeks. The RAGT group underwent 30 min of conventional gait training and an additional 30 min (excluding robot attachment and detachment time) of gait training utilizing an exoskeleton (ANGEL LEGS M20, Angel Robotics, Co, Ltd) in the physiotherapy room. The control group received conventional gait training for the same duration of 60 minas the RAGT group in the physiotherapy room.
Participants
A total of 151 patients with subacute stroke were recruited. Of these, 58 participants were randomized in the RAGT group and 69 in the control group were included in the this prespecified analysis (Fig. 1) (7).
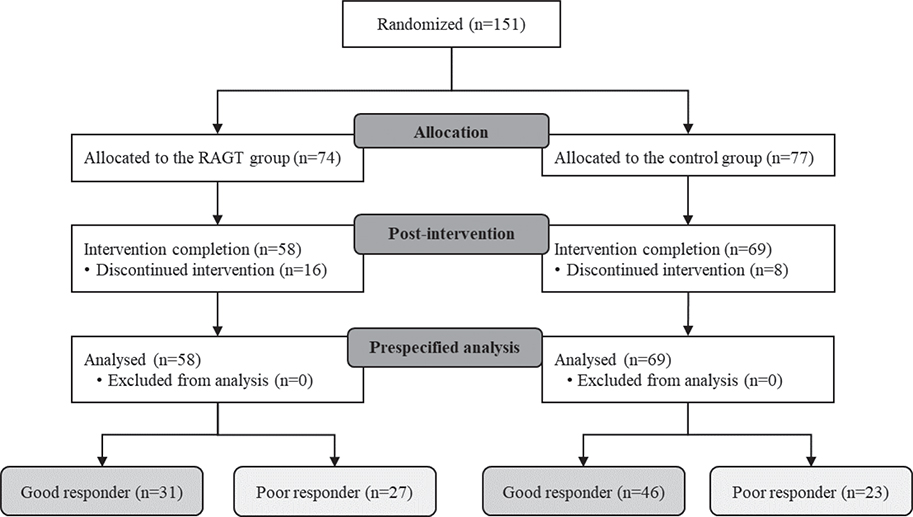
Fig. 1. Flow diagram of a prespecified analysis.
The study enrolled adult patients (aged ≥ 19 years) presenting with hemiparesis following either ischaemic or haemorrhagic stroke. Participants were recruited during the early subacute stage, defined as the period from 7 days to less than 3 months post-onset (9). To be eligible, patients must have been capable of independent ambulation without significant disability prior to the stroke (modified Rankin Scale score ≤ 1) (10). At the time of enrolment, participants were required to demonstrate difficulty with independent gait, defined by a Functional Ambulation Categories (FAC) score of ≤ 2, while maintaining adequate trunk control (Trunk Control Test [TCT] score ≥ 50) (11). Additionally, participants had to meet specific physical criteria to ensure compatibility with the wearable robot: height between 140 cm and 190 cm, weight less than 80 kg, and foot length between 230 mm and 290 mm.
Patients were excluded if they presented with significant difficulties in communication, such as severe cognitive impairment (Mini-Mental State Examination score < 10) (12) or severe speech–language impairment. Other neurological exclusion criteria included ataxia resulting from cerebellar pathway lesions, moderate-to-severe spasticity of the affected lower extremity (Modified Ashworth Scale score ≥ 2) (13), or concurrent neurological disorders affecting ambulatory function (e.g., Parkinson’s disease, multiple sclerosis). Furthermore, patients were ineligible if they had severe lower limb musculoskeletal disorders, contractures limiting range of motion, or an apparent leg length discrepancy of 2 cm or more.
Prespecified analysis
The prespecified analysis evaluated the relationship between potential influencing factors and the achievement of independent gait immediately after the intervention for 4 weeks in each group. Patients were stratified into good and poor responders, defined as whether patients achieved an independent gait. This was defined as the ability to ambulate independently for a distance exceeding 10 m without physical contact, though guidance or monitoring was permitted. This capability was categorized as an FAC score of greater than 3.
The potential influencing factors were selected for this prespecified analysis because they have been found to have some predictive value in previous studies on gait recovery in stroke rehabilitation. For the baseline descriptive characteristics, age, sex, body mass index (BMI), and time since stroke onset were recorded at baseline in each patient (14–17).
At baseline, FAC (18) was used to assess ambulatory function, and the Fugl-Meyer Assessment-Lower Extremity (FMA-LE) (19) and the lower limb score of Motricity Index (MI-LL) (20) were utilized to assess the motor function of the affected lower limb. The assessment of balance function was conducted by TCT and the Berg Balance Score (BBS) (21). In addition, all participants completed self-administered questionnaires with the Geriatric Depression Scale-short form (GDS-SF) (22) and EuroQol-5D (EQ-5D) (23) to assess mood and quality of life at baseline.
Statistical analysis
SPSS version 29.0 (IBM Corp, Armonk, NY, USA) was used for all statistical analyses. The objective of this prespecified analysis was to establish appropriate clinical indications for RAGT by identifying the specific patient subgroups that respond optimally to RAGT and conventional gait training, respectively. Consequently, both groups were subjected to identical analytical methods, and their respective predictive factors were subsequently compared. Good responder and poor responder groups were compared using an independent t-test and χ2 tests for normally distributed variables and Mann–Whitney tests for nonparametric data. No significant outliers were found in the analysis of continuous potential influencing factors. To account for potential multicollinearity among the functional variables (TCT, BBS, FMA-LE, and MI-LL), we employed a multivariate binary logistic regression analysis utilizing the backward elimination method to select the most appropriate independent predictors. Univariate binary logistic regression was conducted to identify possible factors for identifying a good responder to each RAGT and control group and any variables with univariate associations with p-values < 0.20 were considered to be potentially associated with the intervention and were included in a multivariate model. Multivariate binary logistic regression models utilizing the backward elimination method were then developed (24). A p-value < 0.05 was considered to be statistically significant.
RESULTS
Comparison between good and poor responders groups
Baseline characteristics were comparable between the RAGT group and the control group, although the RAGT group exhibited a significantly lower FAC (p < 0.05). Of the 58 patients in the RAGT group and 69 in the control group, 31 (53%) and 46 (67%) patients who reached the independent gait of FAC (≥ 3) were classified as good responders. In contrast, 27 (46%) and 23 (33%) patients were classified as poor responders in the RAGT group and the control group, respectively. There was no significant difference in the rate of the achievement of independent gait between the 2 groups (p = 0.147).
In the RAGT group, FAC, K-MMSE, FMA-LE, and MI-LL at baseline were significantly higher in good responders than in poor responders (p < 0.05). In the control group, FAC, BBS and FMA-LE at baseline were significantly higher in good responders than in poor responders (p < 0.05). In addition, there was a significantly longer duration in good responders than poor responders in the control group (p < 0.05, Table I).
| RAGT group (n = 58) | Control group (n = 69) | ||||||||
| Independent gait (n = 31) | Non-independent gait (n = 27) | p-value | Independent gait(n = 46) | Non-independent gait (n = 23) | p-value | ||||
| Demographic characteristics | |||||||||
| Sex (M:F) | 22:9 | 14:13 | 0.178 | 25:21 | 21:13 | 0.450 | |||
| Age (years) | 60.5 (15.0) | 62.2 (13.5) | 0.660 | 57.2 (11.7) | 62.8 (15.2) | 0.097 | |||
| Height (cm) | 164.7 (8.9) | 162.2 (6.8) | 0.255 | 165.6 (8.4) | 163.3 (9.2) | 0.305 | |||
| Weight (kg) | 64.1 (8.1) | 62.9 (9.8) | 0.626 | 63.5 (10.0) | 58.8 (8.2) | 0.057 | |||
| Body mass index | 23.7 (2.8) | 23.9 (3.6) | 0.773 | 23.1 (3.0) | 22.1 (2.8) | 0.168 | |||
| Hypertension (yes) | 19 | 17 | 1.000 | 25 | 21 | 1.000 | |||
| Diabetes mellitus (yes) | 13 | 5 | 0.087 | 17 | 29 | 0.276 | |||
| Heart failure (yes) | 0 | 0 | 1.000 | 0 | 0 | 1.000 | |||
| Stroke type (ischaemic:haemorrhage) | 20:11 | 19:8 | 0.781 | 28:18 | 11:12 | 0.318 | |||
| Stroke lesion (supratentorial: infratentorial:both) | 24:6:1 | 18:7:2 | 0.608 | 41:4:1 | 18:3:2 | 0.368 | |||
| Stroke duration (days) | 25.2 (20.3) | 34.7 (23.7) | 0.103 | 27.7 (19.9)* | 41.4 (23.9) | 0.015 | |||
| Functional characteristics | |||||||||
| FAC | 1 [0–2]* | 0 [0–2] | 0.020 | 1 [0–2]* | 0 [0–2] | 0.047 | |||
| K-MMSE | 26.6 (3.5)* | 23.0 (6.1) | 0.025 | 23.8 (6.8) | 23.5 (4.7) | 0.141 | |||
| TCT | 77.5 (15.9) | 69.7 (13.2) | 0.096 | 76.7 (16.0) | 69.8 (14.1) | 0.134 | |||
| BBS | 13.7 (12.2) | 8.4 (6.5) | 0.122 | 16.0 (13.8)* | 8.9 (9.8) | 0.024 | |||
| FMA-LE | 18.3 (7.0)* | 13.3 (6.6) | 0.003 | 19.3 (7.6)* | 13.8 (8.8) | 0.011 | |||
| MI-LL | 49.0 (18.2)* | 38.3 (16.6) | 0.029 | 51.3 (19.9)* | 37.0 (15.3) | 0.003 | |||
| GDS-SF | 7.5 (4.4) | 7.3 (4.0) | 0.888 | 6.1 (3.7) | 7.3 (4.7) | 0.297 | |||
| EQ-5D | 0.4692 (0.2683) | 0.4693 (0.2311) | 0.950 | 0.5347 (0.2581) | 0.4546 (0.2635) | 0.215 | |||
| Values are presented as number or mean (SD). RAGT: robot-assisted gait training; FAC: functional ambulatory category; K-MMSE: Korean Mini Mental State Examination; TCT: Trunk Control Test; BBS: Berg Balance Scale; FMA-LE: Fugl-Meyer Assessment-Lower Extremity; MI-LL: lower limb score of Motricity Index; GDS-SF: Geriatric Depression Scale-Short Form: EQ-5D: EuroQal-5D-3L. *. p < 0.05, compared with non-independent gait. |
|||||||||
Influencing factors analysis
Table II presents the results of the univariate and multivariate analysis. In the univariate analysis, stroke duration, FAC, K-MMSE, TCT, BBS, FMA-LE, and MI-LL demonstrated potential associations with the achievement of independent gait in the RAGT group (p < 0.20). On the other hand, the relatively relating factors in the control group were stroke duration, FAC, TCT, BBS, FMA_LE, and MI-LL (p < 0.20). Potential influencing factors with a p-value < 0.2 were then used in the multivariate analysis.
In the multivariate analysis, K-MMSE and MI-LL were significantly independent factors to predict good responders in the RAGT group (p < 0.05, Nagelkerke’s R2 of 0.389). On the other hand, stroke duration and MI-LL were significantly independent factors to predict good responders in the control group (p < 0.05, Nagelkerke’s R2 of 0.411, see Table II).
| Potential influencing factors | RAGT group | Control group | |||||||
| Univariate analysis | Multivariate analysis | Univariate analysis | Multivariate analysis | ||||||
| Exp(β) (95% CI) | p-value | Exp(β) (95% CI) | p-value | Exp(β) (95% CI) | p-value | Exp(β) (95% CI) | p-value | ||
| Demographic characteristics | |||||||||
| Sex | –0.820 (0.149–1.300) | 0.138 | NT | –0.646 (–0.236~1.771) | 0.396 | ||||
| Age | –0.992 (0.986~1.029) | 0.654 | –0.965 (–0.925~1.007) | 0.100 | NT | ||||
| Body mass index | 0.975 (0.826~1.152) | 0.768 | 1.132 (0.948~1.351) | 0.170 | NT | ||||
| Stroke type | 0.766 (–0.253~2.314) | 0.636 | 1.697 (0.618~4.659) | 0.305 | |||||
| Stroke duration | 0.980 (0.956~1.005) | 0.110 | NT | 0.972 (0.949~0.996)* | 0.021 | 0.968 (0.940~0.997)* | 0.031 | ||
| Functional characteristics | |||||||||
| FAC | 3.319 (1.218~9.045)* | 0.019 | NT | 2.090 (1.004~4.351)* | 0.049 | NT | |||
| K-MMSE | 1.168 (1.031~1.325)* | 0.015 | 1.196 (1.044~1.370) | 0.010 | 1.010 (0.931~1.095) | 0.813 | |||
| TCT | 1.038 (1.000~1.078) | 0.051 | NT | 1.031 (0.995~1.068) | 0.088 | NT | |||
| BBS | 1.060 (0.998~1.125) | 0.059 | NT | 1.053 (1.003~1.106)* | 0.039 | NT | |||
| FMA-LE | 1.115 (1.023~1.215)* | 0.014 | NT | 1.089 (1.018~1.165)* | 0.014 | NT | |||
| MI-LL | 1.037 (1.003~1.072)* | 0.030 | 1.045 (1007~1.085) | 0.020 | 1.044 (1.012~1.077)* | 0.007 | 1.050 (1.008~1.094)* | 0.018 | |
| GDS-SF | 1.013 (0.895~1.148) | 0.837 | 0.924 (0.815~1.048) | 0.217 | |||||
| EQ-5D | 0.997 (0.124~8.031) | 0.998 | 3.241 (0.476~22.087) | 0.230 | |||||
| RAGT: robot-assisted gait training; FAC: functional ambulatory category; K-MMSE: Korean Mini Mental State Examination; TCT: Trunk Control Test; BBS: Berg Balance Scale; FMA-LE: Fugl-Meyer Assessment-Lower Extremity; MI-LL: lower limb score of Motricity Index; GDS-SF: Geriatric Depression Scale-Short Form: EQ-5D: EuroQal-5D-3L. *. p < 0.05. | |||||||||
DISCUSSION
This prespecified analysis suggest that the overground RAGT with an exoskeletal wearable robot might be expected to be effective in patients with subacute stroke who have relatively good cognitive function despite a relatively longer stroke duration.
In this study, we found previously reported potential factors influencing ambulatory functional recovery after stroke, because interactions between them are likely and might affect recovery. The recovery of gait function in subacute stroke patients is determined by multifactorial interplay involving baseline stroke severity, initial motor and balance deficits, and cognitive and psychosocial status (25). Specifically, previous meta-analyses have identified stroke duration, TCT, and ML-LL as critical factors in this regard (26). The finding that stroke duration and motricity index were found to be independently significant predictors of independent walking in the control group that received conventional gait rehabilitation therapy in this study is considered to be consistent with existing research. The absence of TCT analysis as a significant predictor in this study is hypothesized to be attributable to the restriction of the study’s participants to patients with relatively preserved trunk control function, all of whom had TCT scores of 50 or higher. In contrast to the group that received conventional gait rehabilitation therapy, ML-LL was found to be an independently significant predictor in the RAGT group that received overground gait training using a wearable exoskeletal robot, similar to the control group. However, cognitive function assessed by K-MMSE was identified as another independently significant predictor, and the exclusion of stroke duration is considered a very meaningful result. Cognitive function is crucial for gait recovery because walking is a complex task demanding attention and executive resources to adapt to environmental changes and perform motor learning (27). A previous study (28) reported a significant correlation between technology acceptance and consistent participation in training, and improved performance. As such, robot-assisted gait training necessitates a higher level of technology acceptance among participants in comparison with traditional gait rehabilitation methodologies. These findings may also be considered a limitation of overground gait training using wearable exoskeletons. The provision of suitable feedback in RAGT is regarded as a domain requiring enhancement to facilitate more effective comprehension and active involvement in robot-assisted gait training by participants.
The exclusion of stroke duration as a significant predictor in the RAGT group is considered a highly interesting result. Stroke duration is a critical determinant for the improvement of gait function because the recovery follows a non-linear, time-dependent trajectory driven by biological mechanisms (29). Because conventional gait rehabilitation is based on activity-dependent plasticity driven by repetitive practice, homeostatic neuroplasticity serves as a crucial mechanism to stabilize neuronal excitability and maintain network equilibrium (30). Therefore, to enhance gait function through the mechanism of homeostatic neuroplasticity, intensive gait rehabilitation should be conducted as early as possible during the subacute stroke phase. These results suggest that stroke duration emerged as a significant negative independent predictor in the control group. In contrast, overground gait training using a wearable exoskeletal robot involves a much higher exercise intensity compared with conventional gait rehabilitation. Consequently, it operates primarily through Hebbian neuroplasticity, achieved by performing correct, repetitive, and active tasks (31, 32). As Hebbian neuroplasticity is largely driven by the intensity and repetition of practice, the specific timing of intervention may have a less restrictive influence compared with spontaneous biological recovery. This mechanism may explain why stroke duration did not emerge as a significant predictor in the RAGT group. Timing remains a critical determinant in treadmill-based RAGT. Recent evidence indicates that patients in the subacute phase demonstrate enhanced neuroplastic responses facilitating functional recovery (33), whereas chronic patients can still achieve meaningful gait improvements, though this often necessitates higher intensity or extended intervention periods to induce changes (3). The findings from previous treadmill-based RAGT studies and this study provide highly significant implications for selecting subjects for overground gait training using wearable exoskeletal robots.
Limitations
A limitation of this study is that it restricted the definition of improved walking function to cases where independent walking was achieved through FAC. When assessing ambulatory patients, it is imperative to consider the normalization of their gait patterns, as opposed to merely evaluating their independent performance. Even in stroke survivors who achieve independent ambulation, persistent gait asymmetry and compensatory kinematic deviations can lead to significantly increased metabolic energy expenditure and secondary musculoskeletal complications, which ultimately limit long-term community participation and increase the risk of falls (34, 35). Consequently, gait pattern considerations assume particular significance in the context of gait rehabilitation during the subacute stroke phase. In addition, given that all subjects were limited to patients with relatively good balance function (TCT ≥ 50), it was not possible to extrapolate the indications for overground gait training using wearable exoskeletal robots to subacute stroke patients with poor balance function. Furthermore, the restriction of the study’s participants to early subacute stroke patients precluded the assessment of the effectiveness of the intervention in stroke patients beyond 3 months post-onset. The finding that stroke duration was not a significant predictor in the RAGT group suggests that overground gait training may offer an extended therapeutic window beyond the early subacute phase. While this study focused on subacute patients, these results support the need for future investigations into the efficacy of this intervention for chronic stroke patients. Consequently, further research is warranted to investigate the underlying mechanisms and potential therapeutic applications of these findings.
Conclusion
The findings of this study suggest that suitable candidates for the overground RAGT using a wearable exoskeletal robot could be early subacute stroke patients (less than 3 months post-onset) with preserved cognitive function, regardless of stroke duration within this timeframe. It is imperative that further research be conducted to ascertain the practical applicability of these findings.
ACKNOWLEDGEMENTS
Ethical clearance: The study has been approved by the Institutional Review Board (IRB) of each hospital (IRB of Severance Hospital, South Korea (IRB no. 1-2021-0031), IRB of National Traffic Injury Rehabilitation Hospital (No. NTRH-21016), IRB of Samsung Medical Center (IRB no. 2021-07-021), IRB of the National Health Insurance Service Ilsan Hospital (No. NHIS- 2021-07-029), and IRB of the Universiti Teknologi MARA (No. REC/04/2021 (MR/26)), and conforms to the Declaration of Helsinki. All the participants provided written informed consent before starting the study procedures.
Trial details: Trial registration: ClinicalTrials.gov identifier: NCT05157347
REFERENCES
- Colombo G, Joerg M, Schreier R, Dietz V. Treadmill training of paraplegic patients using a robotic orthosis. J Rehabil Res Dev 2000; 37: 693–700.
- Chang WH, Kim YH. Robot-assisted therapy in stroke rehabilitation. J Stroke 2013; 15: 174–181. https://doi.org/10.5853/jos.2013.15.3.174
- Mehrholz J, Kugler J, Pohl M, Elsner B. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst Rev 2025; 5: CD006185. https://doi.org/10.1002/14651858.CD006185.pub6
- Morone G, Bragoni M, Iosa M, De Angelis D, Venturiero V, Coiro P, et al. Who may benefit from robotic-assisted gait training? A randomized clinical trial in patients with subacute stroke. Neurorehabil Neural Repair 2011; 25: 636–644. https://doi.org/10.1177/1545968311401034
- Lam T, Pauhl K, Krassioukov A, Eng JJ. Using robot-applied resistance to augment body-weight-supported treadmill training in an individual with incomplete spinal cord injury. Phys Ther 2011; 91: 143–151. https://doi.org/10.2522/ptj.20100026
- Goffredo M, Guanziroli E, Pournajaf S, Gaffuri M, Gasperini G, Filoni S, et al. Overground wearable powered exoskeleton for gait training in subacute stroke subjects: clinical and gait assessments. Eur J Phys Rehabil Med 2019; 55: 710–721. https://doi.org/10.23736/S1973-9087.19.05574-6
- Chang WH, Kim TW, Kim HS, Hanapiah FA, Lee JW, Han SH, et al. Efficacy of wearable exoskeleton for gait recovery in patients with stroke: a multicenter randomized controlled trial. Stroke 2025; 10.1161/STROKEAHA.125.052763. https://doi.org/10.1161/STROKEAHA.125.052763
- Chang WH, Kim TW, Kim HS, Hanapiah FA, Kim DH, Kim DY. Exoskeletal wearable robot on ambulatory function in patients with stroke: a protocol for an international, multicentre, randomised controlled study. BMJ Open 2023; 13: e065298. https://doi.org/10.1136/bmjopen-2022-065298
- Bernhardt J, Hayward KS, Kwakkel G, Ward NS, Wolf SL, Borschmann K, et al. Agreed definitions and a shared vision for new standards in stroke recovery research: the Stroke Recovery and Rehabilitation Roundtable Taskforce. Neurorehabil Neural Repair 2017; 31: 793–799. https://doi.org/10.1177/1545968317732668
- Burn JP. Reliability of the modified Rankin Scale. Stroke 1992; 23: 438.
- Collin C, Wade D. Assessing motor impairment after stroke: a pilot reliability study. J Neurol Neurosurg Psychiatry 1990; 53: 576–579. https://doi.org/10.1136/jnnp.53.7.576
- Kang Y, Na DL, Hahn S. A validity study on the Korean Mini-Mental State Examination (K-MMSE) in dementia patients. J Korean Neurol Assoc 1997; 15: 300–308.
- Blackburn M, van Vliet P, Mockett SP. Reliability of measurements obtained with the modified Ashworth scale in the lower extremities of people with stroke. Phys Ther 2002; 82: 25–34. https://doi.org/10.1093/ptj/82.1.25
- Chang WH, Sohn MK, Lee J, Kim DY, Lee SG, Shin YI, et al. Predictors of functional level and quality of life at 6 months after a first-ever stroke: the KOSCO study. J Neurol 2016; 263: 1166–1177. https://doi.org/10.1007/s00415-016-8119-y
- Morone G, Iosa M, Paolucci T, Muzzioli L, Paolucci S. Relationship between body mass index and rehabilitation outcomes in subacute stroke with dysphagia. Am J Phys Med Rehabil 2019; 98: 608–612. https://doi.org/10.1097/PHM.0000000000001159
- Stinear CM. Prediction of motor recovery after stroke: advances in biomarkers. Lancet Neurol 2017; 16: 826–836. https://doi.org/10.1016/S1474-4422(17)30283-1
- Stinear C. Prediction of recovery of motor function after stroke. Lancet Neurol 2010; 9: 1228–1232. https://doi.org/10.1016/S1474-4422(10)70247-7
- Holden MK, Gill KM, Magliozzi MR, Nathan J, Piehl-Baker L. Clinical gait assessment in the neurologically impaired: reliability and meaningfulness. Phys Ther 1984; 64: 35–40.
- Fugl-Meyer AR, Jaasko L, Leyman I, Olsson S, Steglind S. The post-stroke hemiplegic patient. 1. a method for evaluation of physical performance. Scand J Rehabil Med 1975; 7: 13–31.
- Demeurisse G, Demol O, Robaye E. Motor evaluation in vascular hemiplegia. Eur Neurol 1980; 19: 382–389. https://doi.org/10.1159/000115178
- Jung HY, Park JH, Shim JJ, Kim MJ, Hwang MR, Kim SH. Reliability test of Korean version of Berg Balance Scale. J Korean Acad Rehabil Med 2006; 30: 611–618.
- Lesher EL, Berryhill JS. Validation of the Geriatric Depression Scale – Short Form among inpatients. J Clin Psychol 1994; 50: 256–260.
- Greiner W, Claes C, Busschbach JJ, von der Schulenburg JM. Validating the EQ-5D with time trade off for the German population. Eur J Health Econ 2005; 6: 124–130.
- Mickey RM, Greenland S. The impact of confounder selection criteria on effect estimation. Am J Epidemiol 1989; 129: 125–137. https://doi.org/10.1093/oxfordjournals.aje.a115101
- Veerbeek JM, van Wegen E, van Peppen R, van der Wees PJ, Hendriks E, Rietberg M, et al. What is the evidence for physical therapy poststroke? A systematic review and meta-analysis. PLoS One 2014; 9: e87987. https://doi.org/10.1371/journal.pone.0087987
- Van Criekinge T, Truijen S, Schroder J, Maebe Z, Blanckaert K, van der Waal C, et al. The effectiveness of trunk training on trunk control, sitting and standing balance and mobility post-stroke: a systematic review and meta-analysis. Clin Rehabil 2019; 33: 992–1002. https://doi.org/10.1177/0269215519830159
- Woollacott M, Shumway-Cook A. Attention and the control of posture and gait: a review of an emerging area of research. Gait Posture 2002; 16: 1–14. https://doi.org/10.1016/s0966-6362(01)00156-4
- Comani S, Velluto L, Schinaia L, Cerroni G, Serio A, Buzzelli S, et al. Monitoring neuro-motor recovery from stroke with high-resolution EEG, robotics and virtual reality: a proof of concept. IEEE Trans Neural Syst Rehabil Eng 2015; 23: 1106–1116. https://doi.org/10.1109/TNSRE.2015.2425474
- Preston E, Ada L, Stanton R, Mahendran N, Dean CM. Prediction of independent walking in people who are nonambulatory early after stroke: a systematic review. Stroke 2021; 52: 3217–3224. https://doi.org/10.1161/STROKEAHA.120.032345
- Murphy TH, Corbett D. Plasticity during stroke recovery: from synapse to behaviour. Nat Rev Neurosci 2009; 10: 861–872. https://doi.org/10.1038/nrn2735
- Belda-Lois JM, Mena-del Horno S, Bermejo-Bosch I, Moreno JC, Pons JL, Farina D, et al. Rehabilitation of gait after stroke: a review towards a top-down approach. J Neuroeng Rehabil 2011; 8: 66. https://doi.org/10.1186/1743-0003-8-66
- Kleim JA, Jones TA. Principles of experience-dependent neural plasticity: implications for rehabilitation after brain damage. J Speech Lang Hear Res 2008; 51: S225–239. https://doi.org/10.1044/1092-4388(2008/018)
- Calabro RS, Sorrentino G, Cassio A, Mazzoli D, Andrenelli E, Bizzarini E, et al. Robotic-assisted gait rehabilitation following stroke: a systematic review of current guidelines and practical clinical recommendations. Eur J Phys Rehabil Med 2021; 57: 460–471. https://doi.org/10.23736/S1973-9087.21.06887-8
- Awad LN, Binder-Macleod SA, Pohlig RT, Reisman DS. Paretic propulsion and trailing limb angle are key determinants of long-distance walking function after stroke. Neurorehabil Neural Repair 2015; 29: 499–508. https://doi.org/10.1177/1545968314554625
- Patterson KK, Parafianowicz I, Danells CJ, Closson V, Verrier MC, Staines WR, et al. Gait asymmetry in community-ambulating stroke survivors. Arch Phys Med Rehabil 2008; 89: 304–310. https://doi.org/10.1016/j.apmr.2007.08.142