LETTER TO THE EDITOR
COMMENTS ON: BILATERAL MOVEMENT-BASED COMPUTER GAMES IMPROVE SENSORIMOTOR FUNCTIONS IN SUBACUTE STROKE SURVIVORS: A RANDOMIZED CONTROLLED TRIAL
Simranjot KAUR, BPT, MPT1, Parveen KUMAR, BPT, MPT, PhD2,3, Simranjeet KAUR, BPT, MPT3 and Nidhi SHARMA, BPT, MPT, PhD1*
From the 1Department of Neurological Physiotherapy, Maharishi Markandeshwar Institute of Physiotherapy and Rehabilitation, Maharishi Markandeshwar (Deemed to be University), Mullana-133207, Ambala, 2Pal Physiotherapy Clinic, Ambala City, Haryana and 3Department of Musculoskeletal Physiotherapy, Maharishi Markandeshwar Institute of Physiotherapy and Rehabilitation, Maharishi Markandeshwar (Deemed to be University), Ambala, Haryana, India
Citation: J Rehabil Med 2023; 55: jrm00364. DOI: https://dx.doi.org/10.2340/jrm.v55.4873
Copyright: © Published by Medical Journals Sweden, on behalf of the Foundation for Rehabilitation Information. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Accepted: Nov 15, 2022; Published: Jan 4, 2023
Correspondence address: Dr. Nidhi Sharma. Department of Neurological Physiotherapy, Maharishi Markandeshwar Institute of Physiotherapy and Rehabilitation, Maharishi Markandeshwar (Deemed to be University), Mullana-Ambala, Haryana - 133207, India. E-mail: sharma.nidhi.physio@mmumullana.org; sharmanidhiphysio@gmail.com
The authors of the original article (Lam et al. (1)) were given the opportunity to comment in response to this Letter to the Editor, but chose not to do so.
We read the article by Lam et al. (1), on the use of bilateral movement-based computer games to improve sensorimotor functions in subacute stroke survivors, with great interest. The authors present a well-designed study with interesting findings, and draw the conclusion that bilateral movement-based computer games may serve as an adjuvant to conventional rehabilitation programmes for improving upper limb recovery among stroke survivors. However, we have some difficulty in interpreting their findings.
First, the abstract, does not state the age group and the male:female ratio of study participants, which is a basic requirement of reporting the methods in an abstract (2). Secondly, the keywords do not accord with Medical Subject Headings (MeSH) terms (“subacute stroke survivors; computer gaming”), which is a requirement of the journal guidelines; instead the authors use keywords such as “stroke, video games, exergaming”, etc.
In their introduction, the authors use a 1-tailed hypothesis: “the use of customized bilateral movement-based computer games to improve recovery of the paretic upper limb”. In our view, this should have been a 2-tailed hypothesis, with a statement such as “there may be a significant difference in improvement in sensorimotor functions in subacute stroke survivors” as an alternative hypothesis, and a null hypothesis that “there may not be a significant difference in improvement in sensorimotor functions in subacute stroke survivors”. Despite this, the authors have used a 2-tailed method as input parameters, giving a required sample size of 80 (Fig. 1). For a 1-tailed method, the required sample size would be 62, and, with a drop-out rate of 10%, 68 would be the required sample size (Fig. 2).
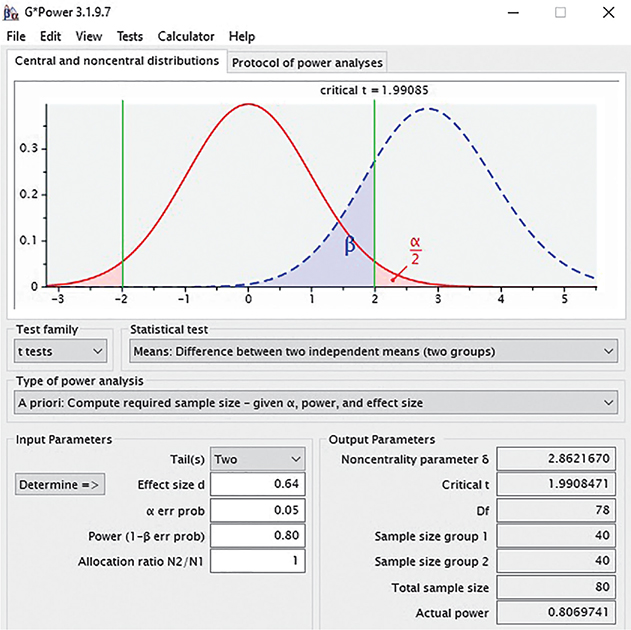
Fig. 1. Sample size estimation (2-tailed).
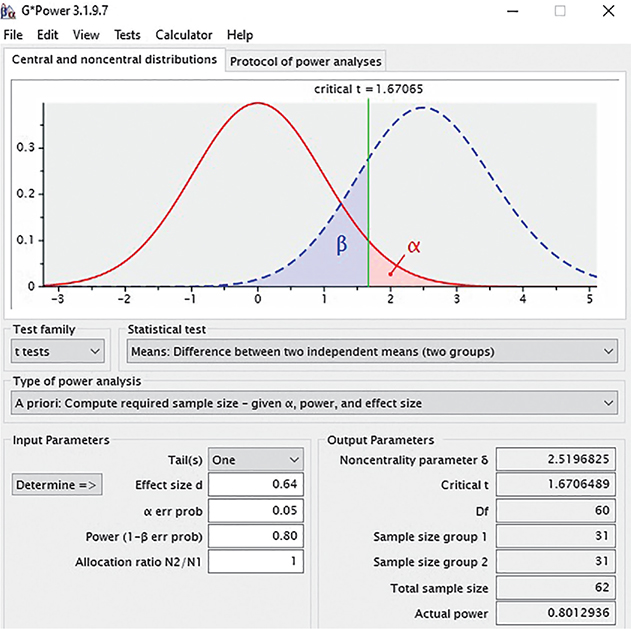
Fig. 2. Sample size estimation (1-tailed).
The methodology of this study is unclear. The study title states that the intervention was given to improve sensorimotor functions. However, the authors do not report any of the treatment interventions and outcome measures for sensory functions. A review has shown a need for more studies to be conducted into sensorimotor training with the use of virtual reality (3).
The study design is not clear; the description in the material and methods section states that the study is a randomized, placebo-controlled, single-blinded clinical trial. However, for a placebo-controlled design, a pre–post-control group design should be used (2).
The description of participants’ characteristics in the material and methods section is also unclear; in the inclusion criteria the duration of stroke is selected as 1 week and 6 months, yet the study focusses on subacute stroke as per the title; hence, the inclusion of 1 week stroke is unexplained. Stroke is divided into the following phases: the first 24 h is considered the hyper-acute phase, 1 week of stroke is classed as the acute phase, the first 3 months duration is classed as the early sub-acute phase, and 4–6 months is classed as the late sub-acute phase. From 6 months onwards, it is called chronic stroke (4).
The authors state that randomization was performed using stratified sampling. Yet, it is not clear whether the stratification was proportionate or disproportionate. In addition, there is no information regarding the male:female ratio of subjects. The authors have not explained why they include a large age range, 45–70 years, in one strata and a small range, 71–85 years, in the other. Since the literature shows 45–60 years of age is classed as middle-aged and 61–85 years as older-adults, the strata could have been selected accordingly (5).
The authors convey that the study was reported under a Consolidated Standards of Reporting Trials (CONSORT) statement, yet the study flow chart provided does not match the one given by the CONSORT statement. We consider that the flowchart of CONSORT 2017 (6) (Non-pharmacological) could have been used (Fig. 3).
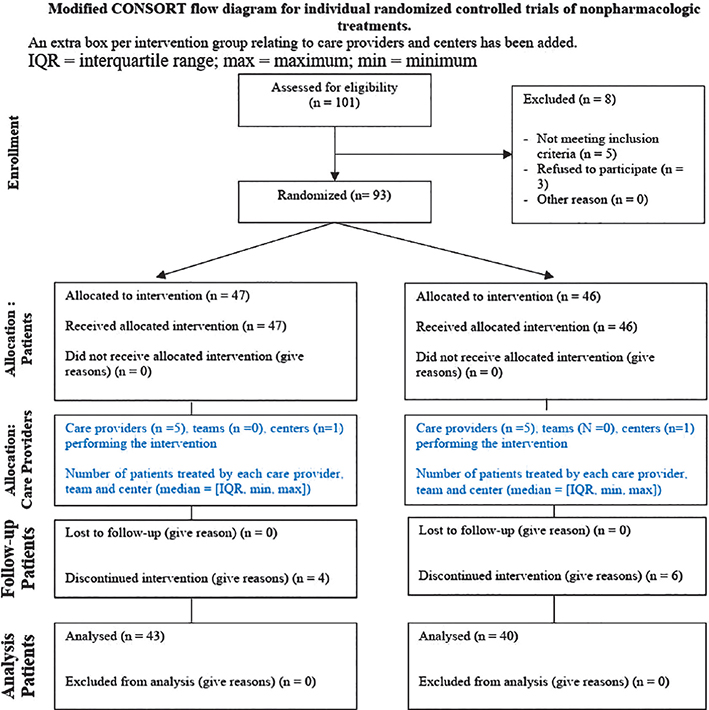
Fig. 3. Consolidated Standards of Reporting Trials (CONSORT) statement flow diagram.
In the results section, the values for minimal clinically important difference (MCID) of each of the outcome measures are suggested to be mentioned for clarity of the significant effect of the intervention on each outcome measure. As per each outcome measure, the suggested MCID value for the Fugl-Meyer Assessment of Upper Extremity (FMA-UE) is 9–10 (6), yet the result shows an MCID of 15.75. The MCID values for the Action Research Arm Test (ARAT) are suggested to be 12–17 (7), yet the results show an MCID of 14.95. The MCID values suggested are 0.8% to 19.5% (8). However, the resulting values are 5.15 kg for grip strength of the paretic side and 1.61 kg for the non-paretic side.
The statistical analysis section does not explain why the Wilcoxon signed-rank test was not used for not normally distributed data if a paired t-test or Student’s t-test was used as parametric test for normally distributed data. Finally, it is not explained why analysis of covariance (ANCOVA) was used instead of a 2-way analysis of variance (ANOVA) (which determines how 2 independent factors interact with one another to affect a dependent variable (2)).
We would be interested in the authors’ thoughts on these comments.
REFERENCES
- Lam SSL, Liu TW, Ng SSM, Lai CWK, Woo J. Bilateral movement-based computer games improve sensorimotor functions in subacute stroke survivors. J Rehabil Med 2022; 54: jrm00307.
- Portney LG, Foundations of clinical research: applications to evidence-based practice. Boston, MA: F.A. Davis; 2020.
- Adamovich S V., Fluet GG, Tunik E, Merians AS. Sensorimotor training in virtual reality: a review. NeuroRehabilitation 2009; 25: 29–44.
- Lee G. Whole-body vibration in horizontal direction for stroke rehabilitation: a randomized controlled trial. Med Sci Monit 2019; 25: 1621–1628.
- Lee SB, Oh JH, Park JH, Choi SP, Wee JH. Differences in youngest-old, middle-old, and oldest-old patients who visit the emergency department. Clin Exp Emerg Med 2018; 5: 249–255.
- Boutron I, Altman DG, Moher D, Schulz KF, Ravaud P. CONSORT statement for randomized trials of nonpharmacologic treatments: a 2017 update and a CONSORT extension for nonpharmacologic trial abstracts. Ann Int Med 2017; 167: 40–47.
- Arya KN, Verma R, Garg RK. Estimating the minimal clinically important difference of an upper extremity recovery measure in subacute stroke patients. Top Stroke Rehabil 2011; 18: 599–610.
- Bohannon, Richard W. Minimal clinically important difference for grip strength: a systematic review. J Phys Ther Sci 2019; 31: 75–78.