ORIGINAL REPORT
PREDICTING INSTITUTIONALIZATION AFTER SUBACUTE STROKE REHABILITATION USING THE 12-ITEM WORLD HEALTH ORGANIZATION DISABILITY ASSESSMENT SCHEDULE
SINIKKA TARVONEN-SCHRÖDER, MD, PHD1 AND MARI KOIVISTO, MSC2
From the 1Neurocenter, Turku University Hospital, Turku, Finland and Clinical Neurosciences, University of Turku, Turku, Finland and 2Department of Biostatistics, University of Turku, Turku, Finland
Objective: To evaluate the utility of the 12-item World Health Organization Disability Assessment Schedule (WHODAS-12) in predicting institutionalization after subacute stroke rehabilitation.
Design: Prospective observational study.
Methods: On a specialized rehabilitation ward, discharge WHODAS-12 scores of 156 consecutive patients (24-h National Institutes of Health Stroke Scale (NIHSS) ≥ 15) and assessment from their proxies were compared, and receiver operating characteristic curves for predicting institutionalization were generated. Clinician-rated assessments of functioning were applied for comparison.
Results: Thirty-three percent of the patients were unfit to respond, due to the consequences of major stroke. However, both patient and proxy WHODAS-12 sum scores differentiated the community (n = 70) and institution (n = 86) groups (p = 0.02 and p < 0.0001, respectively), the discriminative accuracy (area under the curve; AUC) being 0.63 and 0.79, respectively. In proxy assessments, the institutionalized patients were significantly more impaired in all item comparisons except for emotions and concentrating. Ability to participate differentiated the groups as accurately as activities (AUC 0.75 vs 0.78, respectively). The corresponding discriminative accuracy of the clinician-rated World Health Organization (WHO) minimal generic data-set sum score and modified Rankin Scale were 0.74 and 0.79 (p < 0.0001), respectively.
Conclusion: Despite its brevity and subjectivity, the WHODAS-12 from proxies has shown high accuracy in predicting institutionalization after subacute rehabilitation of individuals with major stroke, the impact of participation being as relevant as that of activities.
LAY ABSTRACT
This study investigated the utility of the patient- and proxy-rated 12-item World Health Organization Disability Assessment Schedule (WHODAS-12) in predicting institutionalization after rehabilitation of patients with major stroke. At discharge from rehabilitation, a median of 3 months after stroke onset, 33% of the 156 patients were not fit to respond due to the consequences of major stroke. Both of these brief measures differentiated those discharged to community from those institutionalized. WHODAS from proxies was more accurate in predicting institutionalization, and as accurate as the clinician-rated gold-standard measure, the modified Rankin Scale. Both components of WHODAS, i.e. activities and participation, were equally relevant in differentiating the 2 discharge groups. WHODAS-12 is recommended as part of individualized patient- and family-centered discharge planning after rehabilitation of patients with major stroke.
Key words: institutionalization; rehabilitation; stroke; subacute; WHODAS.
Citation: J Rehabil Med 2023; 55: jrm6531. DOI: https://doi.org/10.2340/jrm.v55.6531.
Copyright: © Published by Medical Journals Sweden, on behalf of the Foundation for Rehabilitation Information. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Accepted: May 31, 2023; Published: Aug 7, 2023
Correspondence address: Sinikka Tarvonen-Schröder, Neurocenter, Turku University Hospital, PO Box 52, FI-20521 Turku, Finland. E-mail: sinikka.tarvonen-schroder@tyks.fi
Competing interests and funding: The authors have no conflicts of interest to declare.
Stroke is the leading cause of adult disability worldwide. Almost half of the annual 12.2 million incident cases of stroke need subacute inpatient rehabilitation (1). After major stroke, the main goal of rehabilitation is discharge back to the community. It is important to identify accurately and efficiently the patients’ discharge disposition to ensure an optimal transition. Holistic approach and patient and family perspectives are essential for a successful outcome when making these decisions. Individualization of assessment, including patient and family perceptions (2, 3), and using self-reported measures (4–6) have been called for. Shifting weight from merely patient-centred to more family-centred operational models (7) would be beneficial, as major stroke affects a large number of people, especially family members. A systematic approach to this group of relatives and caregivers, using reliable and validated instruments, should be developed.
The World Health Organization Disability Assessment Schedule (WHODAS), a generic International Classification of Functioning, Disability and Health (ICF)-based measure, encompassing items from activities and participation, has been validated for stroke (8). The 12-item WHODAS (WHODAS-12) has been shown to correlate strongly with clinician-rated measures of impairment and disability at discharge from subacute stroke rehabilitation (4). The 12-item short version is easy for laypeople to use, thus allowing a prompt survey of patient- and proxy perceptions.
The aim of this study was to evaluate whether WHODAS-12 can be utilized in finding disabilities in participation as well as in activities, and in predicting institutionalization after subacute rehabilitation of individuals with major stroke. To analyse the validity of the results, we also applied 2 clinician-rated assessments of functioning, the WHO minimal generic set covering functioning and health and the modified Rankin Scale for comparison.
PATIENTS AND METHODS
On Turku University Hospital specialised inpatient rehabilitation ward, 156 consecutive patients with major stroke were enrolled between August 2015 and June 2021. The participants gave verbal and written informed consent for the study (19.5.2015, 73/2015). The patients were mostly referred to the neurological rehabilitation unit from the acute stroke unit of the same university hospital. Sometimes the patient had to wait after the acute stroke unit care on a general ward for stabilization of the medical condition before intensive rehabilitation. At discharge, the rehabilitants were divided into 2 groups, those discharged back into the community and those institutionalized, which usually meant discharge to a residential healthcare centre where assisted living residence or other long-term facility was arranged locally. Sometimes, however, the permanent facility was arranged directly from the rehabilitation ward.
Multi-disciplinary team evaluation consisted of assessments made by a neurologist, a physiotherapist, an occupational therapist, a speech and language therapist, a neuropsychologist, a social worker, a rehabilitation planner, rehabilitation nurses and, when necessary, other consultants too. The intensive comprehensive inpatient rehabilitation programme included combined coordinated meetings with these rehabilitation specialists 5 days a week according to patients’ individual needs, in addition to constant daily rehabilitative nursing.
Inclusion criteria of this study were major ischaemic or haemorrhagic stroke, defined as 24-h NIHSS ≥ 15 (9), age over 18 years at stroke onset, premorbid independent living, first time need for inpatient rehabilitation, and ability to sit in a wheelchair for a minimum of 30 min. Exclusion criteria were previous stroke causing permanent disability, current major medical, neurological or psychotic condition in addition to stroke, and medical reasons for interrupted rehabilitation.
Proxies, usually family members or relatives, sometimes a close friend, were encouraged to participate in daily activities, in different therapy and social work sessions and in at least 1 meeting with the entire team to discuss the current medical and functional status of the patient and the future goals and plans including discharge destination. An important part of the rehabilitation programme was a home visit during a weekend at the end of the in-stay, accompanied by caregiver(s) who completed an unofficial questionnaire created by the multi-professional team about the patient’s capabilities and needs during the home stay. In most cases, recurrent home visits could be arranged. Before these weekends at home, a rehabilitation planner made a home visit accompanied by the patient, caregiver(s) and 1 or 2 other members of the multi-professional team in order to secure a safe stay with family members and caregivers.
At discharge, a neurologist assessed functioning using the WHO minimal generic data-set and modified Rankin Scale (mRS). The patients and proxies completed the 12-item patient and proxy WHODAS 2.0. To avoid missing data, in some cases the participants were assisted by a clinician. However, 52 patients were not capable of responding themselves because of cognitive impairment or aphasia. The participants were blinded to each others’ responses.
Socio-demographic data, including age at stroke onset, sex, living situation (cohabiting), years of education and working status (i.e. work or study), were collected from the participants, significant others and hospital medical records. The 24-h NIHSS score after possible thrombolysis and/or thrombectomy was also collected from the medical records. Time from stroke onset to rehabilitation admission and length of stay in rehabilitation were calculated.
Functional variables included WHODAS-12 sum score, item and component scores, the WHO minimal generic data-set score and item scores and mRS score. The 2 discharge groups (community vs institution) were chosen as the dependent outcome variables.
Scales
WHODAS 2.0 (http://www.who.int/classifications/icf/whodasii/en/) is a generic ICF-based measure. The WHODAS-12 includes 12 items from 6 domains in 2 components, i.e. activities: cognition (learning and concentration), mobility (standing and walking), and self-care (washing and dressing oneself) and participation: relationships (dealing with strangers and maintaining friendships), life activities (doing housework and ability to work or study), and social participation (emotional functions and engaging in community). Each of these 12 items is rated according to a 5-point Likert-type scale (either from 1 to 5 or from 0 to 4, the latter being used in the current study). For the ICF classification of disability, the scores were transformed into ICF disability categories, which grade the difficulty experienced by the participant in performing a given activity: 0 means no (0–4%), 1 means mild (5–24%), 2 means moderate (25–49%), 3 means severe (50–95%), and 4 means extreme or complete (96–100%) difficulty in this specific activity.
There are 2 basic options for computing the summary scores for the WHODAS 2.0: simple, when the scores from each of the items are simply added up (10), and complex item-response-theory” (IRT) (11) based scoring, which takes into account multiple levels of difficulty for each WHODAS 2.0 item. In classical psychometric analysis (10), the WHODAS 2.0 structure has been shown to be unidimensional and to have high internal consistency. As a result, the simple sum of the scores of the items across all domains constitutes a statistic that is sufficient to describe the degree of functional limitations. Simple scoring of WHODAS is specific to the sample at hand and should not be assumed to be comparable across populations. In order to compare populations, complex scoring (11) is more useful. This study used the simple scoring in each item and across the total 12 items to ensure an easy visualization of the severity grades rated by the participants using the short, simple and easy WHODAS-12 and to compare these ratings with severities of the other assessments. Thus, the total score of WHODAS was calculated as the sum of all these 12 sub-scores ranging from 0 to 48, with lower scores indicating better functioning. Total scores 1–4 mean mild, 5–9 moderate, and 10–48 severe disability (8, 12, 13). In this study, patient and proxy assessments were made, according to the current functional status at the time of discharge, to investigate the utility of WHODAS at this important real-life situation in subacute stage.
The WHO minimal generic data-set covering functioning and health consists of 7 domains: energy and drive functions, emotional functions, sensation of pain, carrying out daily routine, walking, moving around, and remunerative employment. The scoring system is similar to WHODAS, the scores being transformed to ICF disability categories and the sum score ranging from 0 to 28 (14).
A simple composite tool of activities and participation, mRS, encompasses 7 levels: 0 = independent patients with no residual symptoms, 1 = no significant disability despite symptoms, able to carry out all previous duties and activities, 2 = slight disability, unable to carry out all previous activities, but able to look after own affairs without assistance, 3 = moderate disability, requiring some help but able to walk independently, 4 = moderately severe disability, unable to walk and attend to bodily needs without assistance, 5 = severe disability, bedridden, incontinent and requiring constant nursing care and attention, 6 = death. The mRS has a substantial clinical threshold between each point in the scale and the difference between 1 or more grades is clinically meaningful (6, 15).
Statistical analysis
Descriptive statistics were calculated for all variables and were presented as frequencies and percentages for categorical variables and as medians with range of values and interquartile range (IQR) percentiles for continuous variables. The comparisons between the 2 discharge groups for continuous variables were carried out using χ2 test, or, in case of small frequencies, Fisher’s exact test, and for continuous variables using non-parametric Kruskal-Wallis test. Difference on Hodges-Lehmann estimate for median difference was used. Finally, receiver operating characteristic (ROC) curves using WHODAS, the WHO minimal generic data-set, and mRS scores were generated to compare their discriminative accuracy (area under the curve; AUC) and Youden’s J index applied to calculate the optimal cut-off point on the ROC curve. The proxy WHODAS rating was used, as no proxy responses were missing. p-values < 0.05 (2-tailed) were considered statistically significant. SAS 9.4 for Windows (SAS Institute Inc., Cary, NC, USA) was used for all statistical analyses.
RESULTS
Sociodemographic data for the groups discharged to community (n = 70) and to institution (n = 86) are shown in Table I. The median discharge date was 3 months (85.4 days) after stroke onset.
The median scores, IQR and range of patient (n = 104) and proxy (n = 156) WHODAS-12 sum scores and proxy item and component scores for the 2 discharge groups are shown in Table II. Patient and proxy WHODAS sum score clearly differentiated the 2 groups. In proxy ratings, significant differences between the 2 groups were found in both component and item level comparisons, except for emotional functions and concentrating. Clinically, most significant between-group differences were found in self-care, household activities and joining in community, the institution group being more impaired than the community group. Work/ study was the only item with maximal median score in both groups (Fig. 1). Significant between-group differences were also found in the WHO minimal generic data-set score and in all separate item comparisons, except for emotional functions. MRS score also differentiated the 2 groups.
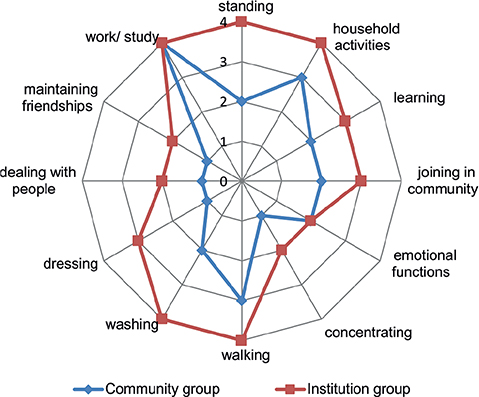
Fig. 1. Median scores of World Health Organization Disability Assessment Schedule (WHODAS) items in community and institution groups assessed by proxies.
ROC curves using WHODAS, the WHO minimal generic data-set, and mRS were generated for comparing the accuracy of these measures for predicting institutionalization. All WHODAS items and both components were statistically significant, except for the items concentrating and emotional functions. WHODAS activities and participation components had equal discriminative accuracy and the same cut-off score. Table III shows the cut-off score on the ROC curve, sensitivity, specificity, and AUC for WHODAS, the WHO minimal generic data-set and mRS.
DISCUSSION
At discharge from rehabilitation of 156 consecutive inpatients a median of 3 months after major stroke, the 12-item patient and proxy WHODAS-12 sum score could differentiate those discharged to community from those institutionalized. However, one-third of the patients were not fit to respond themselves because of the sequelae of major stroke. The predictive accuracy of the proxy WHODAS was high and on an equal level with clinician-ratings using the WHO minimal generic data-set and mRS. On closer scrutiny, all WHODAS proxy items and both components had higher scores denoting more severe disability in the institution group than in the community group, the discriminative accuracy being significant in all items except for concentrating and emotional functions. In predicting institutionalization, ability to participate was as accurate as activities. According to the clinician’s ratings, emotions did not differentiate the 2 groups, either.
Previous studies using instruments of impairment and disability, such as the NIHSS, FIM, Barthel index, Mobility Scale for Acute Stroke, Motor Assessment Scale and Cognitive Screening Test, have also shown the utility of these instruments in predicting discharge dispositions after acute and subacute stroke care and rehabilitation (2, 16–21). These measures, developed for professional use, are time-consuming and do not evaluate participation. As disability after subacute rehabilitation and in later phases of stroke should not be explained solely by the level of dependence in activities of daily living (ADL) or clinical impairment, measures with more diverse domains including participation should also be applied.
The mRS, a widely used tool to assess functioning in subacute stroke, does incorporate aspects of impairment, activity and participation. It has been shown to provide high predictive value for death and disability at 3 months post-stroke, as defined by a mRS score in the range 2–6 (22). However, this measure is extremely crude and does not reveal itemized data. The WHO minimal generic data-set, comprising 7 items of body functions, activities and participation, has been developed to be a starting point for comparisons between different studies and populations (14). It is a generic ICF-based data-set covering functioning and health with the least number of domains of functioning that can be used to explain significant differences between people with various health issues. WHODAS, on the other hand, is a multidimensional measure validated for stroke. It can be used to assess both patient and proxy perceptions and it has been recommended for use in subacute stroke as well as in chronic stroke (4, 23). The 12-item version is easy for laypeople to use.
There is a previous study evaluating WHODAS in predicting institutionalization using the 36-item version (24). In this large Taiwanese register study WHODAS was the only instrument used, and the conclusion was that at least 6 months after stroke the 36-item WHODAS could predict institutionalization of stroke patients. The sum score and the cognition and mobility domain scores, especially, facilitated a moderately high accuracy of discrimination for the risk for institutionalization in a long-term care facility. However, it was pointed out that the responses may have been biased; only patient responses were available or, in case of cognitive impairment, dementia, or aphasia, some caregivers could represent the patients for the interview, which caused inconsistency of subjectivity in the responses. In the current study, a moderately-high to high discriminative accuracy was found in WHODAS-12 items dressing, washing, household activities, joining in community, standing and walking. In both of these studies, life activities and mobility were found to be most impaired in both discharge groups. Closer comparison of the results with those of the Taiwanese study are challenging, as the current study included a highly selected population of inpatients a median 3 months after stroke, while the Taiwanese study encompassed all stroke survivors at least 6 months after stroke. Hence, the distribution of severities of activity limitations and participation restrictions may vary between these 2 populations. In addition, the Taiwanese study analysed WHODAS responses retrospectively and only at the domain level, while the current study analysed responses at the item and component levels at discharge from subacute rehabilitation.
The current study found that patient and proxy WHODAS-12 assessment a median of 3 months after major stroke could predict institutionalization in rehabilitants with baseline NIHSS scores (medians) 19 and 17.5 in institution and community groups, respectively. At discharge, the cut-off score for the proxy WHODAS was 28 and for the patient WHODAS 32, both indicating severe disability, compared with a proxy score of 30 in our previous study in individuals with stroke severity varying from mild to severe (20). The predictive accuracy of WHODAS sum score for institutionalization or community discharge has been found to be moderately-high to high, varying between 0.88 in our previous study in individuals with wider variability in stroke severity (20) and 0.74 in the Taiwanese study (24), being 0.79 in the current study. The corresponding predictive accuracy of the WHO minimal generic data-set and modified Rankin Scale were at the same level, 0.74 and 0.79, respectively. Thus, in the present study, the predictive accuracy of the proxy WHODAS was equal with that of the mRS, the most widely used tool to measure stroke outcome at 3 months after stroke onset; however, the mRS yields no personalized or itemized information for decision-making. Hence, these results, based on all 3 studies, support the utility of WHODAS in predicting discharge disposition post-stroke in the subacute and chronic phase. In the current study, the predictive accuracy of the 2 WHODAS components activities and participation were also high (0.78 and 0.75, respectively), the median score being moderate (2.0 –2.1/ 0–4) in the community group and severe (3.0/ 0–4) in the institution group. The cut-off score was 2.3 for both activities and participation. Thus, ability to participate seems to be as significantly related to discharge disposition as activities, underlining the importance of considering participation in life situations in addition to activities of daily living when planning discharge destination and necessary services.
WHODAS gives valuable information comparing the present functional ability with the functional status before stroke, which is especially important when planning transition from rehabilitation to home/community vs institution. Yet, the 12-item WHODAS instead of the longer version would be preferable in clinical practice, as it is less time-consuming, anticipating better compliance among participants. In individuals with major stroke, proxy perceptions are even more important than in milder severities, as stroke survivors may not be able to respond themselves due to severe cognitive impairment or aphasia. In addition, these proxies are usually the very same people taking care of the patients with stroke after discharge, and their perceptions are often crucial in making future plans and discharge decisions. However, it is noteworthy, that cohabiting (vs living alone) was not statistically significantly associated with discharge destination in the current population, in contrast to several other previous studies (2, 3, 19).
Study limitations
Although the number of participants in the study was limited, it was large enough for the purpose of this research and to achieve useful results. The multidisciplinary inpatient rehabilitation population was selected, hence the results cannot be generalized to all stroke survivors. However, if a measure seems useful in differentiating subgroups in a population with limited functional variability, it also suggests utility in a population with wider functional variability. The data were collected in 1 facility only; medical, social and cultural features may differ worldwide. Nevertheless, WHODAS and the WHO minimal generic data-set have been developed to study comparability across different populations and nations. The application of cross-sectional study design does not allow confirmation of causal relationships of disability, i.e. whether they are based on the disease itself or its secondary consequences. However, the study included only inpatients with premorbid independent living and first-time need for inpatient rehabilitation after major stroke. In closer analyses, only proxy responses were used, as one-third of the patients were not able to respond themselves because of severe cognitive impairment or aphasia. No proxy responses, on the other hand, were missing in this prospective study. Furthermore, proxies are often potential caregivers after discharge, thus, their perceptions are crucial in strengthening family-centred approach, which is recommended, especially after major stroke. Studies that examine discharge destination at a set interval after stroke have the advantage that the predictors are not affected by length of hospitalization and rehabilitation. However, it was decided to investigate the utility of WHODAS at the time of discharge from inpatient rehabilitation, i.e. a real-life situation in clinical practice when the participants already had some experience from community life. The idea was to investigate the utility of WHODAS at the earliest possible time-point after stroke. Hence, WHODAS was applied according to the current functional status at the time of discharge, not in the previous 30 days.
CONCLUSION
In spite of its brevity and subjectivity, the proxy WHODAS-12 has shown high accuracy in predicting institutionalization after subacute rehabilitation of individuals with major stroke, the impact of participation being as relevant as activities.
The predictive accuracy of the proxy WHODAS at a median of 3 months after stroke onset was found to be on an equal level with clinician-rated assessments applying the WHO minimal generic data-set and mRS. After subacute rehabilitation of individuals with major stroke, proxy WHODAS assessment is recommended as part of discharge planning.
ACKNOWLEDGEMENTS
The ethics committee of the university and university hospital approved the study (19.5.2015, 73/2015). The ethics standards of the World Medical Association Helsinki Declaration of 1975, revised in 1983, were followed.
Patients provided informed consent for participation in the research study.
The data associated with the paper are not publicly available, but are available from the corresponding author on request.
REFERENCES
- GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol 2021; 20: 795–820.
- Burton JK, Ferguson EEC, Barugh AJ, Walesby KE, MacLullich AMJ, Shenkin SD, et al. Predicting discharge to institutional long-term care after stroke: a systematic review and metaanalysis. J Am Geriatr Soc 2018;66:161–169. DOI: 10.1111/jgs.15101
- Saab A, Glass-Kaastra S, Young GB. Discharge destination from a rehabilitation unit after acute ischemic stroke. CJNS 2019; 46: 209–215. DOI: 10.1017/cjn.2018.386
- Tarvonen-Schroder S, Hurme S, Laimi K. The World Health Organization Disability Assessment Schedule (WHODAS 2.0) and the WHO Minimal Generic Set of Domains of Functioning and Health versus Conventional Instruments in subacute stroke. J Rehabil Med 2019; 51: 675–682. DOI: 10.2340/16501977-2583
- Vadassery SJ, Kong KH, Ho WML, Seneviratna A. Interview Functional Independence Measure score: self-reporting as a simpler alternative to multidisciplinary functional assessment. Singapore Med J 2019;60:199–201. DOI: 10.11622/smedj.2018048
- Kasner SE. Clinical interpretation and use of stroke scales. Lancet Neurol 2006; 5: 603–612. DOI: 10.1016/s1474-4422(06)70495-1
- Tanwir S, Montgomery K, Chari V, Nesathurai S. Stroke rehabilitation: availability of a family member as caregiver and discharge destination. Eur J Phys Rehabil Med 2014; 50: 355–362. https://pubmed.ncbi.nlm.nih.gov/24518145/
- Kucukdeveci AA, Kutlay S, Yildizlar D, Oztuna D, Elhan AH, Tennant A. The reliability and validity of the World Health Organization Disability Assessment Schedule (WHODAS-II) in stroke. Disabil Rehabil 2013; 35: 214–220. DOI: 10.3109/09638288.2012.690817
- Reznik ME, Yaghi S, Jayaraman MV, McTaggart RA, Hemendinger M, Mac Grory BC, et al. Baseline NIH Stroke Scale is an inferior predictor of functional outcome in the era of acute stroke intervention. Int J Stroke 2018: 13: 806–810. DOI: 10.1177/1747493018783759
- Lord FM, Novick M R, BirnBaum A. Statistical theories of mental test scores. Reading, MA: Addison-Wesley; 1968. https://psycnet.apa.org/record/1968-35040-000
- Rasch G. Probabilistic models for some intelligence and attainment tests. 2nd edition. Chicago: University of Chicago Press; 1980. https://www.abebooks.com/9780226705545/Probabilistic-Models-Intelligence-Attainment-Tests-0226705544/plp
- Andrews G, Kemp A, Sunderland M, Von Korff M, Ustun T. Normative Data for the 12 Item WHO Disability Assessment Schedule 2.0. PloS One 2009; 4: e8343. DOI: 10.1371/journal.pone.0008343
- Üstün TB KN, Chatterji S, Rehm J. Measuring Health and Disability: Manual for WHO Disability Assessment Schedule (WHODAS 2.0). Geneva: WHO; 2010. https://www.who.int/publications/i/item/measuring-health-and-disability-manual-for-who-disability-assessment-schedule-(-whodas-2.0)
- Cieza A, Oberhauser C, Bickenbach J, Chatterji S, Stucki G. Towards a minimal generic set of domains of functioning and health. BMC Public Health 2014; 14: 218. DOI: 10.1186/1471-2458-14-218
- Taylor-Rowan M, Wilson A, Dawson J, Quinn TJ. Functional assessment for acute stroke trials: properties, analysis, and application. Front Neurol 2018; 9: 191. DOI: 10.3389/fneur.2018.00191
- Mees M, Klein J, Yperzeele L, Vanacker P, Cras P. Predicting discharge destination after stroke: a systematic review. Clin Neurol Neurosurg 2016; 142: 15–21. DOI: 10.1016/j.clineuro.2016.01.004
- Thorpe ER, Garrett KB, Smith AM, Reneker JC, Phillips RS. Outcome measure scores predict discharge destination in patients with acute and subacute stroke: a systematic review and series of meta-analyses. J Neurol Phys Ther 2018; 42: 2–11. DOI: 10.1097/npt.0000000000000211
- Brauer SG, Bew PG, Kuys SS, Lynch MR, Morrison G. Prediction of discharge destination after stroke using the motor assessment scale on admission: a prospective, multisite study. Arch Phys Med Rehabil 2008; 89: 1061–1065. DOI: 10.1016/j.apmr.2007.10.042
- Meijer R, van Limbeek J, de Haan R. Development of the Stroke-unit discharge guideline: choice of assessment instruments for prediction in the subacute phase post-stroke. Int J Rehabil Res 2006; 29: 1–8. DOI: 10.1097/01.mrr.0000175269.59788.41
- Tarvonen-Schröder S, Koivisto M. Utility of the World Health Organization Disability Assessment Scale Short Version and the WHO Minimal Generic Data Set covering functioning and health in assessing discharge disposition after sub-acute stroke rehabilitation. Res Rep Med 2020; 3: 1–9. [cited 2020 Dec 14]. Available from: https://escires.com/articles/RRM-3-108.pdf
- Tseng H-P, Lin F-J, Chen P-T, Mou C-H, Lee S-P, Chang C-Y, et al. Derivation and validation of a discharge disposition predicting model after acute stroke. J Stroke Cerebrovasc Dis 2015; 24: 1179–1186. [cited 2015 Apr 03]. Available from: https://www-sciencedirect-com.ezproxy.utu.fi/science/article/pii/S1052305715000142
- Qureshi AI, Chaudhry SA, Sapkota BL, Rodriguez GJ, Suri MF. Discharge destination as a surrogate for Modified Rankin Scale defined outcomes at 3- and 12-months post-stroke among stroke survivors. Arch Phys Med Rehabil 2012; 93: 1408–1413.e1. DOI: 10.1016/j.apmr.2012.02.032
- Küçükdeveci AA, Tennant A, Grimby G, Franchignoni F. Strategies for assessment and outcome measurement in physical and rehabilitation medicine: an educational review. J Rehabil Med 2011; 43: 661–672. DOI: 10.2340/16501977-0844
- Hu HY, Chi WC, Chang KH, Yen CF, Escorpizo R, Liao HF, et al. The World Health Organization Disability Assessment Schedule 2.0 can predict the institutionalization of patients with stroke. Eur J Phys Rehabil Med 2017; 53: 856–862. DOI: 10.23736/s1973-9087.17.04615-9