ORIGINAL REPORT
ONLINE MONITORING OF FOCAL SPASTICITY TREATMENT WITH BOTULINUM TOXIN IN PEOPLE WITH CHRONIC STROKE OR HEREDITARY SPASTIC PARAPLEGIA: A FEASIBILITY STUDY
Hans C. J. W. KERSTENS, MSc1,2, Maarten J. NIJKRAKE, PhD1,3, Bert J. M. DE SWART, PhD1,2, Ria W. G. NIJHUIS-VAN DER SANDEN, PHD1, Marije VOS-VAN DER HULST, PHD4, Gery J. BOS, PhD5, Alexander C. H. GEURTS, PhD1,4 and Philip J. VAN DER WEES, PhD1
From the 1Department of Rehabilitation, Radboud University Medical Center, Nijmegen, The Netherlands, 2Department of Neurorehabilitation, HAN University of Applied Sciences, Nijmegen, The Netherlands, 3Department of Neurology, Donders Institute for Brain, Cognition and Behaviour, Radboud University Medical Center, Nijmegen, The Netherlands, 4Department of Rehabilitation, Rehabilitation center Sint Maartenskliniek, Nijmegen, The Netherlands and 5Department of Rehabilitation, Rehabilitation center Tolbrug, Den Bosch, The Netherlands
Objective: To investigate the feasibility and usability of an online spasticity monitoring tool amongst people with hereditary spastic paraplegia or chronic stroke receiving botulinum toxin treatment, and their healthcare providers.
Methods: Mixed methods cohort study, measuring recruitment success and adherence to the monitoring in 3 rehabilitation institutions. In addition, the System Usability Scale (SUS) and interviews with patients and their healthcare providers were used for quantitative and qualitative analysis, respectively. A deductive directed content analysis was used for qualitative evaluation.
Results: Of the 19 persons with hereditary spastic paraplegia and 24 with stroke who enrolled in the study, recruitment success and adherence were higher amongst people with hereditary spastic paraplegia compared with stroke. Usability was found “marginal” by rehabilitation physicians and “good” by patients and physical therapists (SUS scores 69, 76, and 83, respectively). According to all participant groups, online monitoring potentially contributes to spasticity management if it is tailored to the actual needs and capabilities of patients, and if it can easily be integrated into the daily/working routines of all users.
Conclusion: Online monitoring of spasticity in people with hereditary spastic paraplegia or stroke receiving treatment with botulinum toxin may be feasible, provided that the monitoring tool is tailored to the needs of all users.
LAY ABSTRACT
This study investigated recruitment success and adherence to an online spasticity monitoring tool amongst people with hereditary spastic paraplegia or stroke and their healthcare providers. Usability was evaluated with a questionnaire and interviews. Twenty-four persons with stroke and 19 with hereditary spastic paraplegia participated through 3 rehabilitation institutions. The hereditary spastic paraplegia group was more willing to participate and their adherence to online monitoring was higher than the stroke group. Usability was scored “marginal” by rehabilitation physicians, and “good” by people with spasticity and their physical therapists. The interviews showed that online monitoring may contribute to better spasticity management if it is tailored to the actual needs and capabilities of people with spasticity, and if it can easily be integrated into daily/working routines of all users.
Online monitoring of spasticity seems to be feasible. Tailoring the monitoring tool to patients’ needs and capabilities, and the professionals’ routines may further improve feasibility and usability.
Key words: hereditary spastic paraparesis; spasticity; feasibility studies; internet-based intervention; electronic health record.
Citation: J Rehabil Med 2023; 55: jrm00383. DOI: https://dx.doi.org/10.2340/jrm.v55.6572.
Copyright: © Published by Medical Journals Sweden, on behalf of the Foundation for Rehabilitation Information. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Accepted: Feb 16, 2023; Published: Apr 19, 2023
Correspondence address: Hans C. J. W. Kerstens, Department of Rehabilitation, Radboud University Medical Center, Geert Grooteplein Zuid 10, NL-6525 GA, Nijmegen, The Netherlands. E-mail: Hans.Kerstens@han.nl
Competing interests and funding: The authors have no conflicts of interest to declare.
Although guidelines provide indications for initiating botulinum toxin type A (BoNT-A) injections (1), the timing of subsequent treatment is challenging, because the severity and functional impact of spasticity may vary individually over time. Closely monitoring spasticity may support decision-making in spasticity management for both patients and healthcare professionals.
Spasticity is a prominent feature in many central nervous system disorders, including stroke, spinal cord injury, and hereditary spastic paraplegia (HSP) (2). Pharmacological interventions aim to reduce the complaints and motor problems associated with muscle hypertonia and overactivity (1), either systemically (e.g. oral spasmolysis) or focally (e.g. BoNT-A injections). Together with regular passive stretching of spastic muscles, BoNT-A injections are considered as a mainstay treatment in people who experience spasticity-related complaints and activity limitations (3). BoNT-A treatment is characterized by an initial phase to become effective, a plateau phase with maximum effect, and a wearing-off phase (4).
In addition to experiencing fluctuations in spasticity severity related to the pharmacodynamics of BoNT-A (5), people with spasticity may experience influences of personal and environmental factors, such as fatigue, pain, constipation or temperature changes (6). The progressive (e.g. HSP) or regressive (e.g. stroke) nature of disorders may also cause gradual changes in spasticity severity and impact, which additionally complicates decisions on timing, muscle targeting and dosing of BoNT-A treatment (7, 8). The current study included both people with HSP and people with chronic stroke, as these groups represent different clinical presentations of spasticity in terms of progressiveness, upper-extremity involvement, and severity of spasticity in relation to severity of paresis (9, 10).
Self-monitoring of spasticity may support shared decision-making and improve the timing and execution of BoNT-A treatment. Indeed, the benefits of self-monitoring have been shown in chronic conditions (11, 12). Therefore, we designed a spasticity monitoring tool, consisting of: (i) a commercially available smartphone app (Physitrack® (Physitrack PLC, London) connected to an online platform) to complete a daily self-assessment of spasticity-related symptoms and perceived activity limitations; and (ii) an existing commercially available online platform (Physitrack®) for healthcare professionals to consult the sampled app-data. The spasticity monitoring tool aims to provide insight into the course of individual complaints and activity limitations, in order to empower self-management, shared decision-making, and timing of subsequent BoNT-A treatment. The spasticity monitoring tool is explained in detail in Appendix S1.
This study aimed to investigate the feasibility and usability of the developed spasticity monitoring tool in people with HSP or stroke who already receive BoNT-A treatment. Specific research questions were: (i) what is the recruitment success for using the spasticity monitoring tool in terms of the number of enrolled eligible people in both groups?; (ii) what is the adherence of people with HSP or stroke to using the smartphone app?; (iii) what is the usability of the monitoring tool according to people with HSP or stroke and their healthcare providers (medical rehabilitation specialists and primary care physical therapists)?; and (iv) in what way does the monitoring tool contribute to spasticity management according to people with HSP or stroke and their healthcare providers?
METHODS
Design and setting
In this prospective multicentre cohort study, people with HSP or chronic stroke who were already on BoNT-A treatment for reducing spasticity-related complaints and activity limitations were eligible for inclusion. They were recruited through the outpatient clinic of 3 rehabilitation facilities in the Netherlands (Radboud University Medical Center Nijmegen, Rehabilitation center Tolbrug Den Bosch, and the Rehabilitation center of the Sint Maartenskliniek Nijmegen) between December 2019 and April 2021. They started using the smartphone app immediately after they received their first subsequent BoNT-A treatment and were followed up for 2 full cycles of BoNT-A treatment, which was a period of approximately 6 months, depending on the individual treatment cycle. Healthcare professionals were able to read out the sampled data from the smartphone app in the online platform. A concurrent mixed methods approach was used to measure feasibility (quantitatively) and usability (both quantitatively and qualitatively) (Fig. 1). The study protocol was approved by the regional medical ethics committee (registration number 2019-5466). Data from the online spasticity monitoring tool was stored and reported according to the Declaration of Helsinki (13) and the FAIR principles (Findable, Accessible, Interoperable, Reusable data) (14).
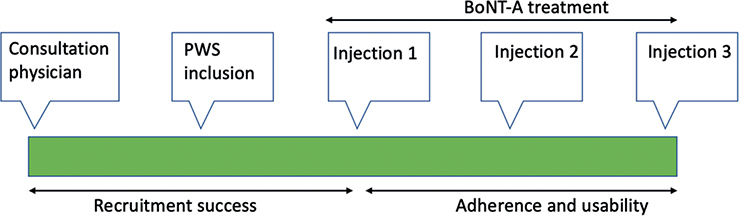
Fig. 1. Study timeline. BoNT-A: botulinum toxin type A; PWS: people with spasticity.
Participants
Three types of participants were included. People with chronic spasticity caused by either a pure form of HSP or stroke were eligible when they met the following criteria: a diagnosis of pure HSP or stroke (≥ 6 months post onset), age ≥ 18 years, with spasticity-related complaints and/or activity limitations, being already on BoNT-A treatment and scheduled for subsequent BoNT-A injections. Exclusion criteria were: inability to communicate in Dutch, cognitive impairments that might impact independent reflection on experiences with the online app during an interview (e.g. severe aphasia or memory deficits), not possessing (or being able to use otherwise) a tablet/smartphone or regular internet connection. The other participant groups consisted of the medical rehabilitation specialists (physicians) who were treating the included patients in the 3 participating rehabilitation facilities (n=8), and the primary care physical therapists who were guiding the exercises of the people with spasticity in the home situation.
This study aimed to include 25 persons with pure HSP and 25 persons with chronic stroke and all of their involved medical rehabilitation specialists and primary care physical therapists.
Recruitment procedure
During the consultation at the outpatient clinic, the medical rehabilitation specialists checked whether the persons scheduled for BoNT-A treatment met the inclusion criteria. These people were then provided with written information about study goals and procedures and invited to participate. If a person, after a minimal reflection period of 2 weeks, was still interested in participating, the primary researcher (HK) called the patient by telephone to verify the inclusion criteria, provide additional information upon request, and answer any remaining questions. Prior to participation, all participants gave their written informed consent. They were all allowed to withdraw from the study thereafter, without giving a reason and without any consequence for their treatment.
After a person was included, the treating medical rehabilitation specialist was notified and requested to participate. In addition, when involved, the primary care physical therapist was informed about the study goals and procedures and was also asked to participate, but therapist participation was not mandatory for a patient being able to participate in the study. All healthcare providers received written information about the study.
Study procedure
All people with spasticity started using the online app on the first day after the first, subsequent BoNT-A treatment and stopped using the online app on the day of the third subsequent BoNT-A cycle. Thus, 2 full cycles of BTX treatment were captured (Fig. 1). All people with spasticity received an individual username and password from the primary researcher (HK) to be able to enter data through the online app. Entering data into the smartphone app took approximately 2 min. The healthcare providers were informed that they had the opportunity to access their patients’ online platform at any time. They were also provided with an individual username and password. All participants received a digital and a paper version of the user manual of the spasticity monitoring tool. In addition, they had the opportunity to contact a helpdesk by phone or email, if needed. The helpdesk was available during office hours and responded to questions within 1 working day. One week after the first BoNT-A treatment, each person with spasticity was phoned by the helpdesk to verify whether they were able to use the smartphone app and access the online platform as they wished.
Outcomes
Feasibility outcomes. Feasibility was evaluated with the following quantitative outcomes: recruitment success, reasons for non-participation, and adherence to using the spasticity monitoring tool. Recruitment success and reasons for non-participation were assessed at 3 levels by calculating:
- the proportion of people with spasticity invited for participation: the number of invited people was divided by the number of potentially eligible people; reasons for not inviting eligible people to join the study were documented by the medical rehabilitation specialist were documented during the first outpatient consultation.
- the proportion of people with spasticity that agreed to participate: the number of people that signed the informed consent was divided by the number of invited people; reasons for non-participation were documented by the primary researcher (HK).
- the proportion of participating primary care physical therapists: the number of therapists that signed the informed consent was divided by the number of invited therapists; reasons for non-participation were documented by the primary researcher (HK).
Adherence to using the smartphone app was calculated for a period of 2 cycles of botulinum toxin: the number of completed daily self-assessments was divided by the expected number of self-assessments per person (i.e. the number of days included in the 2 consecutive BoNT-A cycles). Based on their adherence, people with spasticity were classified as a user (adherence >75%) or a limited/non-user (adherence <40%). These opposite groups in terms of adherence were identified to select patients for the individual interviews, as described in the next paragraph.
Usability outcomes. After the third botulinum toxin injection, usability of the smartphone app was quantitatively assessed by all people with spasticity using the System Usability Scale (SUS). Usability of the online platform amongst the individual medical rehabilitation specialist and primary care physical therapist was quantitatively assessed with the SUS after study completion of their last participating patient. The SUS is a subjective measure consisting of 10 questions, each using a 5-point Likert scale, ranging from score 1 (strongly disagree) to score 5 (strongly agree) (15). The SUS is a validated measure for which a sum score (range 0–100) is considered “unacceptable” when below 50, scores between 50 and 69 are considered “marginal”, and scores 70 or higher are considered to indicate “good” usability (16). In addition to the SUS, 3 self-constructed questions were asked to all participants: (i) “Would you recommend the spasticity monitoring tool to other people with spasticity?” and (ii) ‘Would you recommend the spasticity monitoring tool to other healthcare professionals?’ For these questions a 5-point Likert scale was used with the above-mentioned scoring options. The third question (“Which grade of appreciation do you give the monitoring tool?”) was answered using a 10-point scale (ranging from score 1 “unsatisfactory” to 10 “excellent”).
Perceived usability for and contribution to spasticity management of the spasticity monitoring tool were qualitatively assessed through individual interviews. Because of the COVID-19 pandemic regulations during this study, each individual interview was conducted online (using the platform LifeSize® (Lifesize Video Conferencing, Austin)) instead of a face-to-face interview as initially intended.
Based on the adherence rates, this study purposively sampled 9 persons with HSP or stroke from the user- and limited/non-user groups (17). In addition, all participating medical rehabilitation specialists from the 3 centres involved (n = 8) and all primary care therapists who returned the SUS questionnaire were invited for an individual online interview. Therapists who did not return the SUS questionnaire were called by the primary researcher (HK) to inquire whether they had used the online platform. Those who confirmed they had used the online platform were briefly asked to share their experiences concerning usability. Therapists who had not used the online platform at all were briefly asked to mention the most important reason for non-use.
All individual interviews lasted approximately 30 min and were conducted by the primary researcher (HK) using a semi-structured interview guide. The interview guide was developed by the research team, and shared in advance by email with the participants to optimize their focus on usability topics (18). The following topics were addressed:
- To what extent is the spasticity monitoring tool suitable to monitor the time course of spasticity?
- To what extent did the spasticity monitoring tool provide insight in the course of spasticity and the optimal timing of BoNT-A injections?
- How did the spasticity monitoring tool impact on self-management and shared decision-making?
- Which barriers and facilitators for using the spasticity monitoring tool did you experience?
- Were the items of the self-assessment relevant for evaluating severity and functional impact of spasticity?
Data analysis
Descriptive statistics were calculated for the feasibility outcomes and the quantitative usability outcomes. This analysis was performed using SPSS (IBM Corp. Released 2017, IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY, USA: IBM Corp.).
The qualitative interviews were audio-recorded, verbatim transcribed by a research assistant (MR), and imported into a software management package for the analysis of qualitative data (AtlasTi, version 8.1.27.0, Scientific Software Development GmbH, Berlin, Germany).
AtlasTi was used to perform a deductive, directed content analysis (19), which means that the transcripts were coded according to an a priori formulated theoretical framework of categories, based on the Consolidated Framework for Implementation Research (CFIR). The CFIR supports identifying potential influences on implementation in the 5 domains: intervention, inner setting, outer setting, individuals involved, and process of implementation (20). After coding of the first transcript, the primary researcher (HK) and 1 of the supervisors (MN) discussed the content and coding process. After consensus, the second and third transcripts were coded, and discussed by both researchers. The ordering of the preliminary themes was initially discussed by HK and MN, followed by a discussion with the entire research team until consensus was reached on the final themes.
RESULTS
Recruitment success
Between December 2019 and September 2020, 161 unique consultations of people requiring botulinum toxin treatment were recorded at the outpatient clinics of the 3 participating centres (Radboudumc n = 79, Tolbrug n = 62, and Sint Maartenskliniek n = 20). Of these, 50 persons were excluded because they did not have a diagnosis of HSP or stroke. Another 24 persons were not included because they did not fulfil the other inclusion criteria or because they met the exclusion criteria. Out of 87 eligible persons, 43 were eventually enrolled (24 stroke, 19 HSP) (see Fig. 2). Their characteristics are shown in Table I.
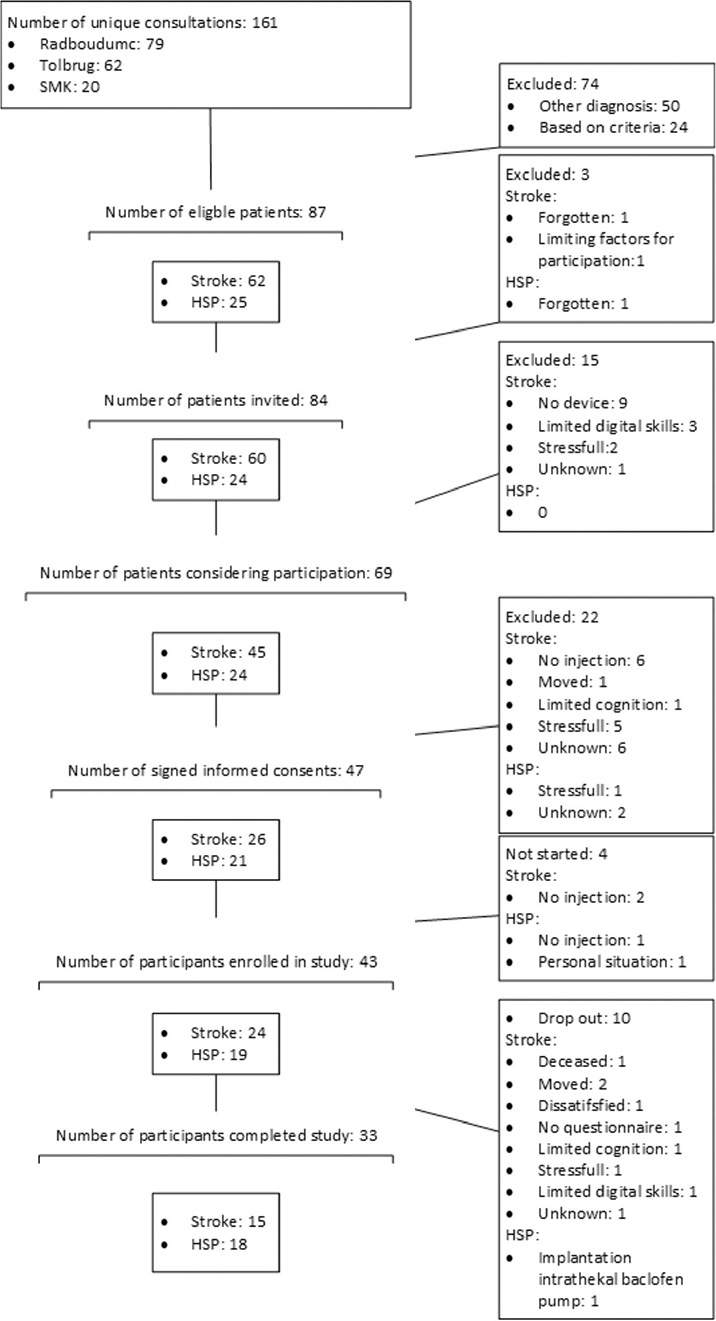
Fig. 2. Flowchart of participants with spasticity from recruitment until completion of the study. HSP: Hereditary Spastic Paraplegia; SMK: Sint Maartenskliniek.
Non-participation occurred more often among people with stroke compared with HSP for the following reasons: not having a smartphone, not knowing how to use the smartphone app, participation being too stressful, and change of treatment plan.
Of the 43 participating people with HSP or stroke, 35 were consulting a primary care physical therapist, of whom 29 therapists (83%; representing 29 patients) were willing to participate. Reasons for non-participation of therapists were: increased workload (n = 4), limited digital skills (n = 1), or unknown (n = 2). Of the 29 included therapists, 18 completed the study. Reasons for therapist drop-out were patient drop-out (n = 9) or miscommunication (n = 2). All 8 medical rehabilitation specialists involved agreed to participate.
Adherence to using the smartphone app
The study intended to sample 2 full injection cycles, which would correspond to minimally 6 consecutive months. Unfortunately, directly after participant recruitment had started, the COVID-19 pandemic struck the Netherlands, which led to frequent postponement of BoNT-A injections. Rescheduling of appointments was not automatically communicated with the researcher, which resulted in the monitoring window sometimes having started before the first injection and ended relatively early. Since we were interested in the adherence over a prolonged period, we decided to set the sampling period for every participant to 24 weeks, as this sampling period was used as a default by the online app provider. This strategy implied that a maximum of 168 daily self-assessments were collected per patient.
As depicted in Fig. 2, 33 patients completed the study (18 patients with HSP, 15 with stroke). Reasons for not completing the study were both frequent and variable in people with stroke, whereas only 1 person with HSP dropped out, due to implantation of an intrathecal baclofen pump. The median overall adherence to using the online app in terms of number of completed daily self-assessments was 49%, which was higher for people with HSP (median 63%) than for people with stroke (median 20%) (Table II).
| Stroke (n = 15) | HSP (n = 18) | ||
| Percentiles | 25 | 0.03 | 0.33 |
| 50 | 0.20 | 0.63 | |
| 75 | 0.61 | 0.90 | |
| HSP: hereditary spastic paraplegia. | |||
Quantitative results for usability
SUS response rates were 60% for people with spasticity (38% stroke and 89% HSP) vs 50% for medical rehabilitation specialist and 24% for primary care physical therapists (Table III). Reasons for not using the online platform by medical rehabilitation specialists were: limited time/workload, technical problems, maternity leave/holidays, change of tasks, or misconception about the availability of the monitoring tool. Reasons for non-use by the other participants was not inquired for and thus remained unknown. From the participants who completed the SUS, people with spasticity had a mean score of 76 points, medical rehabilitation specialists 69 points, and primary care therapists 83 points. The majority of the responding participants stated that they would recommend other people with spasticity and healthcare professionals to make use of the spasticity monitoring tool.
Qualitative results for usability
Nine persons with spasticity (6 with stroke, of whom 3 were non-users and 3 users, and 3 with HSP, all users), all 8 medical rehabilitation specialists who recruited the patients, and 6 primary care physical therapists who completed the SUS were interviewed. From these interviews, a total of 291 unique codes were extracted and categorized into 3 themes: timing of monitoring, experienced benefits, and needs for improvement. Quotes (Q) of participants that exemplify the 3 themes are shown in Table IV.
Timing of monitoring. People with spasticity had different thoughts about the usefulness of the smartphone app. Some felt they did not need it, whereas others experienced clear advantages (Q1). In general, monitoring was experienced as most useful at the start of the BoNT-A injections to establish the initial and subsequent need and timing of BoNT-A continuation. For some, monitoring at a later stage was considered redundant. This view was also expressed by some medical rehabilitation specialists. A more intensive information exchange at the start of the BoNT-A treatment would support adequate spasticity management in terms of indication and timing. One of the rehabilitation specialists suggested using the spasticity monitoring tool before the start of the BoNT-A treatment, thus creating a baseline that might help to assess the initial effects. Primary care physical therapists generally expressed a lower need for monitoring as they felt they had frequent contacts with the patients, providing them with “a clear clinical picture” regarding the course of spasticity (Q2).
Experienced benefits. All people with spasticity valued the daily self-assessment, because they were better able to relate the fluctuations in the visual graphs of their symptoms and activity limitations to the timing of the injection cycles or to other spasticity influencing factors. One of them thought it would be better to ask for the frequency of stumbling than for fall incidents (Q3). Some medical rehabilitation specialists reviewed the online platform data before clinical consultation, which was valued by their patients (Q4). The experiences of the medical rehabilitation specialists themselves were diverse. Some reported that spasticity fluctuations were difficult to associate with the injection cycles, sometimes due to missing values, whereas others expressed that use of the online platform clearly supported clinical decision-making and shared responsibility between physicians and patients. One medical specialist reported the need for a satisfaction score in addition to a change score (Q5). Most primary care physical therapists were very pleased with the availability of daily stretching exercises through the online app. They were generally less focused on the use of the online monitoring platform. Their experiences with the online platform were diverse. Some did not use the online platform data at all, whereas others used it as a starting point to get a clearer clinical picture, based on the patients’ narrative and physical examination. One therapist used the online platform data as a benchmark for his own findings to support spasticity management (Q6).
Need for improvement. Some people with spasticity experienced the use of the smartphone app as tedious. Moreover, they felt that the predefined symptom and activity scores were insufficiently tailored to their individual problems. A few persons stated that they were glad when the sampling period had finished, because it confronted them too much with their problems or because they were tired at the end of the day (Q7).
According to the medical rehabilitation specialists, important improvements would be: easier accessibility, better arrangement and adjustability of the visual graphs, integrated use of the data during the actual clinical consultation, and implementing individual treatment goals within the online platform data. Both medical rehabilitation specialists and primary care therapists mentioned that they would have appreciated the integration of the online platform with the regular electronic patient file, and the possibility to also add relevant data themselves to the patient’s platform in support of shared decision-making (Q8).
All participants would have appreciated personal face-to-face instructions instead of instructions by mail or telephone. They would also have liked to receive automatic notifications to support consistent use of the spasticity monitoring tool.
DISCUSSION
The results of this study show that monitoring spasticity with a tool including a smartphone app and an online platform is feasible and potentially useful. People with stroke typically experience more barriers than people with HSP with regard to using the online monitoring tool as their participation, adherence and response rates were much lower. Based on the people with spasticity who returned the SUS, the usability of the online app and platform would be good, but the large proportion of people who did not return the SUS imposes serious bias, particularly in people with stroke. The same bias is true for the responding therapists reporting high scores for usability. In contrast, the medical rehabilitation specialists all responded to the SUS, indicating marginal to good usability. Qualitative analysis, however, still yielded many suggestions for improvement of usability of the spasticity monitoring tool, particularly from the perspective of patients and medical specialists. In their view, monitoring should be tailored to individual needs, integrated into the routines of all users, and incorporated into the electronic health records.
Recruitment success and adherence
Recruitment success and adherence to online monitoring were much higher for people with HSP compared with stroke. Cognitive limitations and participation being considered too stressful accounted for a lot of non--participants with stroke. Cognitive impairments may also have played a role in the low adherence rates in people with stroke, while the higher adherence by people with HSP may be explained by the fact that the study only included individuals with a pure form of HSP who typically have no cognitive impairments. People with HSP may also have been more motivated, because spasticity is a key problem regarding their daily functioning and also shows a progressive character. In contrast, people with stroke often experience paresis and loss of muscle control to be the most dominant motor problems in terms of their daily functioning, while spasticity may be moderate or even regressive. In their systematic review, Block et al. showed that remote monitoring of physical activity across a variety of neurological diseases was feasible, even in people with impaired cognition (21). Only a minority of their data showed no correlation between activity count and person-reported severity of symptoms. Reduced adherence was found in some of the included studies (21), but dropout rates were lower than in the current study. An important difference compared with the study of Block, is that in our study, we used a device that automatically stored but did not sample data. Patients had to enter a daily self-assessment themselves, which was bothersome for some. Using individually tailored patient-relevant outcomes, which could be sampled by a well-tolerated device, may potentially increase adherence to online monitoring of spasticity, particularly in people with stroke.
Usability and contribution to spasticity management
Regarding usability, the current study showed SUS scores ranging from marginal (medical rehabilitation specialists) to good (people with HSP and stroke, and primary care physical therapists). The good scores of therapists may have been caused by the fact that the Physitrack® app was developed primarily for physical therapists and was adapted to their working routines. In contrast, the medical rehabilitation specialists had to use the online platform next to their electronic health record, which required additional time during the clinical consultations. Indeed, the lack of integration of the online platform with the electronic health record and the necessity to follow several steps to gain access to the preferred visual graphs imposed an extra workload.
According to many participants, monitoring spasticity fluctuations is more helpful in an early stage of botulinum toxin treatment than in a later phase when individual treatment responses and spasticity fluctuations are better known both to patients and to their healthcare providers. Nevertheless, even “experienced” people with spasticity and BoNT-A treatment may face new situations in which it might be useful to intensify spasticity monitoring; for instance, in the case of intercurrent co-morbidity, change of (oral) medication, or when the efficacy of treatment seems to attenuate. A temporary period of close monitoring of spasticity might help to adequately adjust spasticity management to the actual demands of the person. In people with chronic obstructive pulmonary disease, cerebral palsy, or chronic heart failure, self-monitoring has shown to be effective in detecting relevant changes in health status (12), reducing long-term complications (11), and reducing healthcare utilization (22). It is therefore likely that shared decision-making in spasticity management can be improved when self-monitoring is used in critical periods of treatment, tailored to patient-relevant outcomes and combined with systematically sampled data by healthcare professionals.
Adopting a new element in spasticity management, such as online monitoring, requires that all users are convinced of the relevance and usability of the monitoring tool. For example, explaining the benefits of monitoring, matching expectations, sharing tips and tricks with “super-users”, may all contribute to adoption. Having the possibility to send regular reminders, add background information, upload videos for movement analysis, put markers in graphs to identify important events, or zoom in and out of graphs by adjusting the timeline, may further add to the usability of online monitoring. Most importantly, monitoring should be incorporated into the daily routines of all users. Implementation of online monitoring should therefore be prepared carefully, by analysing barriers and the context of users, and tailoring the intervention to individual needs and possibilities of users. Using the CFIR framework is helpful to identify potential barriers for implementation of a new intervention across multiple contexts (20).
Strengths and limitations
The current study has several strengths. It tested the online monitoring tool in a realistic setting. The 3 participating rehabilitation facilities were allowed to follow their own protocols and workflows. In addition, the study provided support via a helpdesk and phoned people with spasticity 1 week after the start of data sampling, but purposely refrained from sending regular reminders as this would have influenced the spontaneous adoption process.
A major limitation of this study is the selection bias that occurred due to non-participation, non-adherence, and non-response, particularly in the stroke population. In addition, the study did not record participant characteristics or adherence for the medical rehabilitation specialists or primary care physical therapists. Moreover, these healthcare providers were able to consult the data entered into the online platform by people with spasticity, but they were unable to enter relevant data themselves due to the inherent technical limitations of the tool used. This may have reduced their perceived relevance and usability and may have weakened the interaction between healthcare professionals and patients.
CONCLUSION
Monitoring of spasticity-related symptoms and activity limitations by means of a monitoring tool with an online app linked to a commercially available online platform seems to be feasible and useful for people with hereditary spasticity (pure HSP) more than for people with stroke. Adequate individual user selection and focused timing of use, together with tailoring the monitoring to individual needs, integrating it into daily routines, and incorporating sampled data into electronic health records may further improve usability and the likelihood of clinical implementation.
Two main clinical messages can be formulated. First, using patient-relevant outcomes tailored to individual needs may enhance adherence to online monitoring of spasticity. Second, tailoring the intensity and period of self-monitoring to individual needs may improve spasticity management in the early and chronic phases of spasticity treatment.
ACKNOWLEDGEMENTS
This work was supported by a PhD grant of the HAN University of Applied Sciences to the first author. This investigation was further supported by an unrestricted grant from Ipsen Pharma. We would like to thank Mees Rekers and Dorien Kil for their contribution to this research.
REFERENCES
- Williams G, Singer BJ, Ashford S, Hoare B, Hastings-Ison T, Fheodoroff K, et al. A synthesis and appraisal of clinical practice guidelines, consensus statements and Cochrane systematic reviews for the management of focal spasticity in adults and children. DisabilRehabil 2022; 44: 509–519. DOI: 10.1080/09638288.2020.1769207.
- Pandyan AD, Gregoric M, Barnes MP, Wood D, Van Wijck F, Burridge J, et al. Spasticity: clinical perceptions, neurological realities and meaningful measurement. Disability and rehabilitation 2005; 27: 2–6. DOI: 10.1080/09638280400014576
- Esquenazi A, Novak I, Sheean G, Singer BJ, Ward AB. International consensus statement for the use of botulinum toxin treatment in adults and children with neurological impairments–introduction. European journal of neurology: the official journal of the European Federation of Neurological Societies 2010; 17: 1–8. DOI: 10.1111/j.1468-1331.2010.03125.x.
- Demetrios M, Khan F, Turner-Stokes L, Brand C, McSweeney S. Multidisciplinary rehabilitation following botulinum toxin and other focal intramuscular treatment for post-stroke spasticity. The Cochrane database of systematic reviews 2013; 6. DOI: 10.1002/14651858.CD009689.pub2.
- Bakheit AM. The pharmacological management of post-stroke muscle spasticity. Drugs & aging 2012; 29: 941–947. DOI: 10.1007/s40266-012-0034-z.
- Gracies JM. Pathophysiology of spastic paresis. II: Emergence of muscle overactivity. Muscle & nerve 2005; 31: 552–571. DOI: 10.1002/mus.20285.
- Kerstens HCJW, Satink T, Nijkrake MJ, De Swart BJM, Nijhuis-van der Sanden MWG, Van der Wees PJ, et al. Experienced consequences of spasticity and effects of botulinum toxin injections: a qualitative study amongst patients with disabling spasticity after stroke. Disability and rehabilitation 2021; 43: 368$1–$2695. DOI: 10.1080/09638288.2020.1746843.
- Kerstens HCJW, Satink T, Nijkrake MJ, De Swart BJM, Van Lith BJH, Geurts ACH, et al. Stumbling, struggling, and shame due to spasticity: a qualitative study of adult persons with hereditary spastic paraplegia. Disability and rehabilitation 2020; 42: 3744–3751. DOI: 10.1080/09638288.2019.1610084.
- Fink JK. Hereditary spastic paraplegia: clinico-pathologic features and emerging molecular mechanisms. Acta Neuropathologica 2013; 126: 307–328. DOI: 10.1007/s00401-013-1115-8.
- Hankey GJ. Stroke. Lancet 2017; 389: 641–654. DOI: 10.1016/S0140-6736(16)30962-X.
- Elkamil AI, Andersen GL, Hagglund G, Lamvik T, Skranes J, Vik T. Prevalence of hip dislocation among children with cerebral palsy in regions with and without a surveillance programme: a cross sectional study in Sweden and Norway. BMC musculoskeletal disorders 2011; 12: 1–7. DOI: 10.1186/1471-2474-12-284.
- Colantonio S, Govoni L, Dellaca RL, Martinelli M, Salvetti O, Vitacca M. Decision Making Concepts for the Remote, Personalized Evaluation of COPD Patients' Health Status. Methods of information in medicine 2015; 54: 240–247. DOI: 10.3414/ME13-02-0038.
- Williams JR. The Declaration of Helsinki and public health. Bulletin of the World Health Organization 2008; 86: 650–651. DOI: S0042-96862008000800022.
- Wilkinson MD, Dumontier M, Aalbersberg IJ, Appleton G, Axton M, Baak A, et al. The FAIR Guiding Principles for scientific data management and stewardship. Scientific data 2016; 3: 1–9. DOI: 10.1038/sdata.2016.18.
- Borsci S, Federici S, Lauriola M. On the dimensionality of the System Usability Scale: a test of alternative measurement models. Cognitive processing 2009; 10: 193–197. DOI: 10.1007/s10339-009-0268-9.
- Bangor A, Kortum PT, Miller JT. An empirical evaluation of the System Usability Scale. International Journal of Human–Computer Interaction 2008; 24: 574–594. DOI: 10.1080/10447310802205776.
- Moser A, Korstjens I. Series: Practical guidance to qualitative research. Part 3: Sampling, data collection and analysis. The European journal of general practice 2018; 24: 9–18. DOI: 10.1080/13814788.2017.1375091.
- Krueger RA, Casey MA. Focus groups a practical guide for applied research. 5th ed. Los Angeles: SAGE Publications Inc.; 2015.
- Berg BL, Lune H. Qualitative research methods for the social sciences. 8 ed. New Jersey: Hanson, K.; 2012.
- Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implementation science 2009; 4: 1–15. DOI: 10.1186/1748-5908-4-50.
- Block VA, Pitsch E, Tahir P, Cree BA, Allen DD, Gelfand JM. Remote Physical Activity Monitoring in Neurological Disease: A Systematic Review. PloS one 2016; 11: e0154335. DOI: 10.1371/journal.pone.0154335.
- Bashi N, Karunanithi M, Fatehi F, Ding H, Walters D. Remote Monitoring of Patients With Heart Failure: An Overview of Systematic Reviews. Journal of medical Internet research 2017; 19: e18. DOI: 10.2196/jmir.6571.
- van Lith BJH, Kerstens HCJW, van den Bemd LAC, der Sanden MWGN, Weerdesteyn V, Smeets RJEM, et al. Experienced complaints, activity limitations and loss of motor capacities in patients with pure hereditary spastic paraplegia: a web-based survey in the Netherlands. Orphanet journal of rare diseases 2020; 15: 1–10. DOI: 10.1186/s13023-020-1338-4.