SHORT COMMUNICATION
ADHERENCE TO A WEB-BASED EXERCISE PROGRAMME: A FEASIBILITY STUDY AMONG PATIENTS WITH HIP OR KNEE OSTEOARTHRITIS
Kenth Louis JOSEPH, MSc1,2, Hanne DAGFINRUD, PhD1, Kåre Birger HAGEN, PhD3, Kristine Røren NORDÉN, MSc1,4, Camilla FONGEN, MSc1, Ole-Martin WOLD, MSc5, Rana S. HINMAN, PhD6, Rachel K. NELLIGAN, PhD6, Kim L. BENNELL, PhD6 and Anne Therese TVETER, PhD1
From the 1Norwegian National Advisory Unit on Rehabilitation in Rheumatology, Center for treatment of Rheumatic and Musculoskeletal Diseases (REMEDY), Diakonhjemmet Hospital, 2Faculty of Medicine, Institute of Health and Society, University of Oslo, 3Division of Health Service, Norwegian Institute of Public Health, 4Norwegian National Unit for Rehabilitation for Rheumatic Patients with Special Needs, Center for Treatment of Rheumatic and Musculoskeletal Diseases (REMEDY), Diakonhjemmet Hospital, 5Norwegian Rheumatism Association, Oslo, Norway and 6Centre for Health, Exercise and Sports Medicine, Department of Physiotherapy, School of Health Sciences, Faculty of Medicine Dentistry & Health Sciences, The University of Melbourne, Melbourne, Australia
Objectives: To describe adherence to a 12-week web-based aerobic exercise programme, to compare characteristics between those who adhere or not, and to identify barriers for exercising in patients with hip or knee osteoarthritis.
Design: Single-arm feasibility study.
Subjects: Patients with hip or knee osteoarthritis in specialist healthcare, age 40–80 years, and not candidates for joint surgery.
Methods: Adherence to a 12-week exercise programme was defined as having completed ≥ 2 exercise sessions a week for at least 8 weeks. Baseline differences between adherent and non-adherent groups in demographics, symptoms, disability, physical activity and fitness were assessed using Mann–Whitney U or χ2 tests. Reasons for not completing exercise sessions were reported in weekly diaries.
Results: A total of 29 patients (median age 64 years, 72% female) were included. Median baseline pain (numerical rating scale 0–10) was 5. Fifteen patients adhered to the exercise programme, 14 did not. Non-adherent patients were less active (p = 0.032) and had lower cardiorespiratory fitness (p = 0.031). The most frequently reported barrier to exercising was sickness. Less than 10% reported pain as a barrier.
Conclusion: Half of the patients with hip or knee osteoarthritis adhered to the digitally delivered exercise programme and the most frequently reported barrier for adherence was sickness, while less than 10% reported pain as a reason for not exercising.
Trial registration: ClinicalTrials.gov, NCT04084834. The Regional Committee for Medical and Health Research Ethics South-East, 2018/2198.
LAY ABSTRACT
Exercise is a core element in the management of osteoarthritis, and adherence to exercise is important to achieve beneficial health effects. Many patients find it challenging to exercise by themselves and need tight support. However, this need cannot solely be met within the healthcare system, and alternative ways to support patients are needed. The aim of this study was to assess adherence to a web-based aerobic exercise programme and to identify barriers for exercising. This feasibility study included 29 participants. Of these, 15 adhered to the programme (exercised at least 2 times per week for a minimum of 8 weeks). Those who did not adhere had lower activity and fitness levels before the start of the study. Sickness was the most frequently reported barrier to exercising, while few reported pain as a barrier. In conclusion, web-based delivery can be valuable in supporting adherence to exercise in patients with hip or knee osteoarthritis.
Key words: exercise; adherence; osteoarthritis; management; web-based; barriers; motivation; digital technology.
Citation: J Rehabil Med 2023; 55: jrm7139. DOI: https://doi.org/10.2340/jrm.v55.7139.
Copyright: © Published by Medical Journals Sweden, on behalf of the Foundation for Rehabilitation Information. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Accepted: Jun 28, 2023; Published: Aug 14, 2023.
Corr: Kenth Louis Joseph, Norwegian National Advisory Unit on Rehabilitation in Rheumatology, Center for Treatment of Rheumatic and Musculoskeletal Diseases (REMEDY), Diakonhjemmet Hospital, Oslo, Norway. E-mail: Kenth-Louis.Joseph@diakonsyk.no
Competing interests and funding: The authors have no conflicts of interest to declare.
Exercise is recognized as an important part of the treatment plan for a wide range of chronic diseases, for curbing symptoms as well as for reducing comorbidities (1). For musculoskeletal diseases such as osteoarthritis (OA), numerous studies have shown beneficial effects of supervised exercise, and adherence to prescribed exercise is associated with reduced joint pain, improved physical function and better health-related quality of life (2).
Evidence supports exercise as a core component in the management of people with OA (3). To obtain beneficial health effects of exercise programmes, adherence is crucial (2), but it is reported that many patients do not adhere to prescribed exercise programmes (4). Long-term adherence to a prescribed exercise programme depends on a range of factors influencing motivation, capability, and opportunity for participating in exercise (5). Current evidence shows that barriers to exercise adherence include patients’ uncertainties about the cause of pain and worries that exercise can cause harm (6). These barriers can be overcome by facilitators, such as tailored exercise programmes, reassurance about the safety and value of exercise, along with encouragement, feedback, and support from healthcare providers (6). A challenge is, however, that the need for long-term individual supervision and support for this large and increasing patient group cannot be met solely within the healthcare system. Development of alternative delivery and follow-up methods is therefore required, and digital technologies (i.e. phone-, SMS-, app- or web-based) for delivery of self-management and exercise programmes may represent a more sustainable way to support patients with life-long need for management (7).
Adherence to exercise is important for gaining and maintaining positive health effects and is therefore a prerequisite for considering “exercise as medicine” (2). Web-based exercise programmes may be a sustainable tool in long-term management of people with OA, but more insight is needed into how patients adhere to such programmes. Hence, the aims of this study were to describe adherence to a 12-week, web-based aerobic exercise programme, to compare characteristics between those who adhered to the programme and those who did not, and to identify barriers for completing exercise sessions in patients with hip or knee OA.
METHODS
Design and participants
The data are collected in a study assessing feasibility of a web-based aerobic exercise programme for patients with OA (8). The exercise programme and methods of delivery are described in detail elsewhere (8). Patients aged 40–80 years, referred to Diakonhjemmet Hospital, Oslo, Norway for surgical consultation due to hip or knee OA, were eligible if not considered candidates for surgery. Exclusion criteria were inability to understand or write Norwegian, to walk unaided and continuously for 15 min, contradictions to maximal exercise testing and inability to access the internet. Forty-nine patients received verbal and written information about the study and 35 were enrolled (Fig. 1).
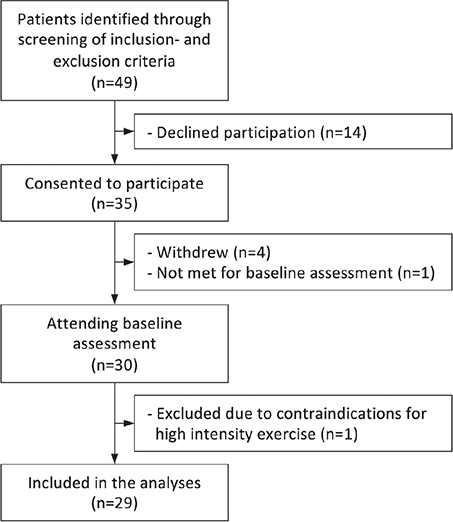
Fig. 1. Study flowchart of patient recruitment and patients included in the analyses.
Data collection and intervention
Patients who consented to participate were asked to complete an electronic questionnaire including demographics (age, sex, body mass index (BMI), education, employment status, living alone/together with someone, smoking, comorbidity), symptoms and disability (troublesome joints, Hip Disability and Osteoarthritis Outcome Score (HOOS) or Knee Injury and Osteoarthritis Outcome Score (KOOS) (0–100, 100 = no disability) (www.koos.nu), and pain (numerical rating scale (NRS) 0–10, 0 = no pain). Physical activity (moderate to vigorous, min/day) was measured by a hip-worn accelerometer (ActiGraph GT3X+, Pensacola, FL, USA). The patients were asked to wear the accelerometer during all waking hours for 7 consecutive days (except during water-based activities). A valid recording is referred to as at least 4 days with minimum 10 h of recording per day (8). In addition, baseline assessments included a maximal modified Balke test (n = 20) or a submaximal single-stage test (n = 9) to assess cardiorespiratory fitness (VO2peak/max) (8), and questions about physical activity habits and pain during physical activity, which were used to determine each patient’s initial exercise level (described elsewhere (8)).
The 12-week web-based programme was developed in close collaboration with a patient organization (Norwegian Rheumatic Association, Oslo, Norway) and was designed as a progressive aerobic exercise programme comprising 3 sessions per week (2 interval and 1 light to moderate intensity session) across 5 different exercise levels. For each increment in exercise level, the weekly exercise dosage was increased (duration and/or intensity using the Borg Rating of Perceived Exertion ranging from 6 (no exertion) to 20 (maximal exertion) (9) as guidance (8). The exercise level for the subsequent week was determined by the project manager based on number of sessions completed and reported barriers for not completing the exercise programme (barriers selected from a predefined list (10) and reported in the electronic exercise diary). If the patient reported to have completed all 3 exercise sessions, the exercise level was increased every other week until the highest level was reached. If exercise sessions were not completed, the same exercise level was sustained for the subsequent week. The exercise programme was e-mailed to the patients at the beginning of each week together with contact information to peer supporters and a tailored message addressing any exercise barriers reported in the diaries. An additional facilitator message designed to encourage weekly exercise adherence (10) was e-mailed to the patient in the middle of the week. After 12 weeks, the patients answered a follow-up questionnaire, and their cardiorespiratory fitness and physical activity level were reassessed.
Adherence
Adherence to the exercise sessions was collected through the weekly electronic exercise diary, including the patients’ reporting of completed exercise sessions and the intensity for each session using the Borg Scale. Adherence to the 12-week programme was defined as having completed ≥ 2 exercise sessions per week (according to the prescribed Borg intensity) for at least 8 weeks (11). Patients not submitting any exercise diaries were categorized as non-adherent.
Barriers to adherence
Patients who completed ≤ 2 of the prescribed sessions in each week were asked to select 1 or more reasons for not completing all 3 sessions. The predefined reasons (“forgot”, “too tired”, “joint hurts so I cannot exercise”, “worried exercise is causing pain/injury”’, “exercise does not help”, “boring”, “lack of time”, “life stress”) are common barriers identified for patients with OA, and conform with a theory-supported behaviour change programme for people with OA (10). An additional “none of the alternatives apply to me” with a free-text option was added.
Statistical analysis
Data are presented as median and interquartile range (IQR, 25th and 75th percentile) or frequencies and percentage. Adherence to the exercise programme is shown graphically. Mann–Whitney U test or χ2 were used to examine differences between the adherent and non-adherent groups in baseline demographics, OA-related symptoms and disability, cardiorespiratory fitness, and physical activity level. Reported barriers are shown graphically. Significance level was set to p < 0.05. IBM SPSS Statistics version 27 was used for statistical analyses.
RESULTS
In total, 29 patients were included in the analyses. Twenty-nine patients had valid accelerometer recordings (mean 6.1 (SD 1.0) days). After the 12-week intervention, 15 patients were categorized as adhering to the exercise programme and 14 were categorized as not adhering (Fig. 2).
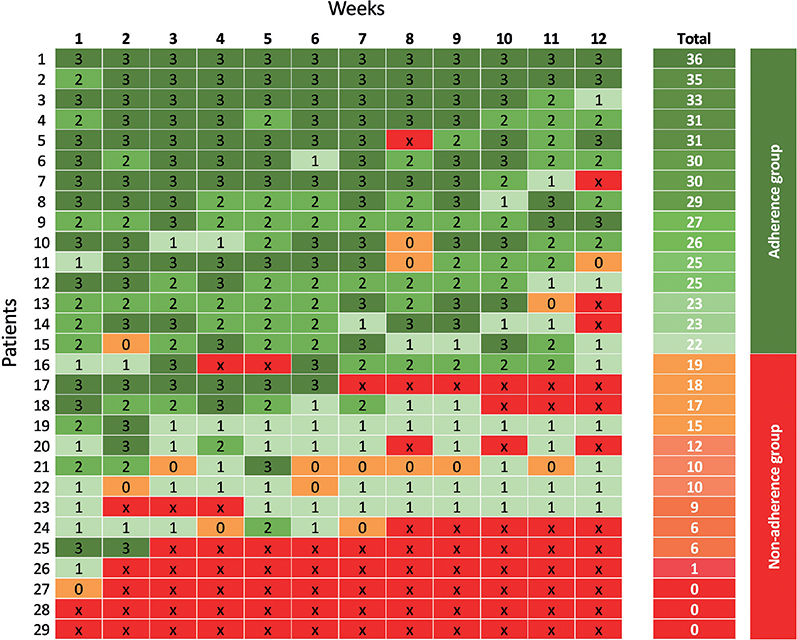
Fig. 2. Individual patient adherence/non-adherence profiles, where the number in the cell refers to the number of exercise sessions completed each week (and in total), and × indicates that the exercise diary was not submitted (= categorized as no exercise sessions completed).
Due to the COVID-19 (SARS-CoV-2) pandemic, 4 patients discontinued the programme: 2 ended at 10 weeks (categorized into the adherent group), and 2 did not fulfil the criteria for adherence.
Baseline characteristics are shown in Table I. The median age of the sample was 64 years, the majority (72%) were female and 79% were overweight/obese (BMI ≥ 25 kg/m2). The patients reported moderate pain level (in the last week) with a median NRS score of 5. The adherent- and non-adherent groups were similar at baseline with the exception that more patients in the non-adherent group reported living alone (p = 0.007), and patients in the adherent-group were more active (p = 0.032) and had better cardiorespiratory fitness (p = 0.031) (Table I).
| Characteristics | All (n = 29) | Adherence group (n = 15) | Non-adherence group (n = 14) | p-value |
| Age, years, median (IQR) | 64 (59–70) | 63 (51–67) | 67 (60–73) | 0.15 |
| Females, n (%) | 21 (72) | 10 (67) | 11 (79) | 0.47 |
| BMI (kg/m2), median (IQR) | 28.3 (25.3–34.6) | 28.0 (25.7–32.1) | 29.1 (24.3–39.3) | 0.57 |
| Education (≥ 1 year of college/university), n (%) | 18 (62) | 9 (60) | 9 (64) | 0.81 |
| Fulltime employment, n (%) | 13 (45) | 8 (53) | 5 (36) | 0.34 |
| Living alone, n (%) | 11 (38)a | 2 (13)a | 9 (64) | 0.007 |
| Non-smoker, n (%) | 28 (97) | 14 (93) | 14 (100) | 0.33 |
| Proportion with comorbidity, n (%) | 19 (68) | 9 (60) | 10 (71) | 0.52 |
| OA-related symptoms | ||||
| Most troublesome joint, n (%) | ||||
| Hip (right/left) | 4 (14) | 2 (13) | 2 (14) | 0.94 |
| Knee (right/left) | 25 (86) | 13 (87) | 12 (86) | |
| Proportion with additional troublesome joint (hip/knee/ankle/hand), n (%) | 23 (79) | 13 (87) | 10 (71) | 0.31 |
| Proportion using daily pain medication, n (%) | 12 (41) | 6 (40) | 6 (43) | 0.88 |
| Pain last week (NRS 0–10, 0 = no pain) | 5 (3–7) | 5 (3–6) | 4 (3–7) | 0.66 |
| Disease activity last week (NRS 0–10, 0 = no disease activity) | 5 (4–7) | 5 (4–7) | 4 (3–7) | 0.30 |
| Fatigue last week (NRS 0–10, 0 = no fatigue) | 2 (0–6) | 3 (0–7) | 2 (0–5) | 0.49 |
| Hip/knee OA symptoms and disability (HOOS/KOOS) | ||||
| Symptoms (0–100, 100 = best score) | 46 (36–61) | 46 (39–64) | 43 (35–59) | 0.54 |
| Pain (0–100, 100 = best score) | 58 (44–72)a | 58 (44–72) | 58 (42–69)a | 0.73 |
| Function in daily living (0–100, 100 = best score) | 63 (55–75) | 63 (61–74) | 68 (38–83) | 0.97 |
| Function in sport and recreation (0–100, 100 = best score) | 25 (13–50) | 35 (17–50) | 25 (8–50) | 0.50 |
| Hip/knee related quality of life (0–100, 100 = best score) | 44 (31–47) | 31 (25–44) | 44 (36–52) | 0.26 |
| Moderate to vigorous physical activity (min/day), median (IQR) | 27 (12–39) | 31 (25–46) | 19 (3–28) | 0.032 |
| Cardiorespiratory fitness (VO2peak/max), median (IQR) | 28.5 (22.8–31.3) | 29.3 (26.0–33.2)b | 23.7 (20.2–30.8)c | 0.031 |
| aMissing, n = 1. bPerformed submaximal cardiorespiratory fitness test, n = 4. cPerformed submaximal cardiorespiratory fitness test, n = 5. IQR: interquartile range; BMI: body mass index; NRS: numerical rating scale; HOOS: Hip Disability and Osteoarthritis Outcome Score; KOOS: Knee Injury and Osteoarthritis Outcome Score; VO2peak/max: peak/max oxygen uptake. p-values analysed by Mann–Whitney U test or χ2 test. Results in bold font are statistically significant. |
||||
Across the 12 weeks, a possible total of 348 diaries could be returned, and a total of 266 were received. Of the 152 diaries asking for barriers for exercising, 124 were returned with “none of the alternatives applies to me” option selected most often. Among the free-text answers, sickness was reported most frequently and less than 10% reported OA joint pain as a barrier (Fig. 3).
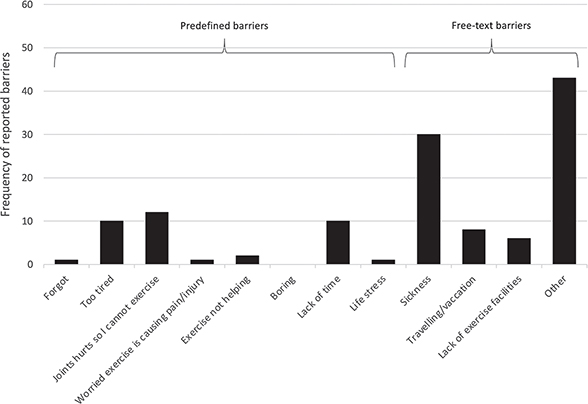
Fig. 3. Reported barriers for completing ≥ 3 exercise session/week, shown by predefined barriers and free-text (“none of the alternatives applies to me”) barriers reported in open ended text (n = 124). In 28 diaries, no barriers were reported.
DISCUSSION
The exercise intervention in this study was delivered during the COVID-19 pandemic, inducing some situation-specific barriers for many patients, but still, half of the OA patients referred for surgical consultation adhered to the web-based exercise programme. Patients in the adherent group were significantly more physically active and had better cardiorespiratory fitness at baseline than the non-adherent group. Less than 10% of the participants reported OA-related pain as a barrier for adherence to exercise.
Adhering to exercise over time is of vital importance for patients with OA, as an action to reduce disease symptoms as well as to reduce risk of comorbidity. Measuring adherence is, however, complex, and comparison of adherence rates between studies is difficult due to lack of standardization of measuring methods and inconsistency of definitions and registration of adherence (12). Self-reporting in diaries is a common method for reporting adherence, and by use of weekly reporting in the current study, the adherence rate was found to be comparable to the results of an 8-week physiotherapist-guided strengthening exercise study (13).
Although the sample size does not allow generalizing of results, all participants were referred to surgical consultation in specialist healthcare and they therefore probably share some common characteristics, such as disease severity. Despite that the current intervention was carried out during the COVID-19 pandemic, half of the patients adhered to the digitally-delivered programme, indicating that this method can be regarded a sustainable follow-up alternative. If approximately half of the patients can follow a digitally delivered programme, extra resources may be allocated to patients who are non-adherent. Based on the current study, people with poor physical fitness or reporting low physical activity may be more prone to be non-adherent.
Exercise is recommended as first-line treatment for patients with OA (3). For obtaining optimal health benefits from exercising (“exercise as medicine”), individual adoption of the programme (including progression of the workload) and sufficient adherence to the programme are needed. An advantage with web-based delivery is the possibility of e-mail automatically triggered by the lack of response, reminding people to submit their diary and pro-actively sending them a facilitator message. Patients at risk for dropping out can be identified, and automatically approached and motivated to continue exercising. Furthermore, the patient-reported exercise diaries provide data on number of fulfilled exercise sessions, intensity and total workload, creating a basis for developing individual progression algorithms, ensuring correct dosage for optimal health benefit for the individual patient. Exploiting advantages of web-based delivery of treatment and support programmes must be part of the future research agenda in the field of chronic diseases.
Support to overcome barriers is an important aspect of facilitating uptake and adherence to exercise (6). However, the current study showed that our predefined barriers provided for reporting in the exercise diary had limited relevance for our sample of participants. This finding was supported in another study of patients with OA (14), indicating that barriers to exercise are varied and diverse and that strategies to overcome barriers must be tailored to the individual in order to maximize success. The most common barrier reported in free-text in the current study was sickness, which may partly be explained by the ongoing COVID-19 pandemic.
This study has some limitations. The feasibility design and the absence of a control group do not allow for confirmative causal conclusions, and the modest sample size limits the generalizability of the results and implies low statistical power for detecting differences in patient characteristics between the 2 groups. The submaximal test is known to overestimate fitness level in those who are less fit (15). However, as more patients in non-adherent group (n = 5) performed the submaximal test compared with the adherent group (n = 4), combining the tests most probably does not inflate the results. Furthermore, there is potential for misclassification of participants who did not return diaries and were classified as non-adherent, as they may have exercised without submitting the diary. Direct comparison with other studies is difficult due to different programmes and methods.
A strength of the study was that patient representatives were involved in the development of the programme, which probably increased the relevance and suitability and, in turn, may have positively influenced adherence.
In conclusion, half of the patients with hip or knee OA adhered to the digitally-delivered exercise programme, indicating that web-based exercise delivery can be valuable in supporting adherence to exercise programmes for patients with hip or knee OA. The most frequently reported barrier for adherence to exercise was sickness, while less than 10% reported joint pain as a reason for not adhering. Patients with low levels of physical activity and physical fitness may be at risk of non-adherence to web-based programme delivery.
ACKNOWLEDGEMENTS
The project was funded by foundation DAM, Oslo, Norway (2019/FO247595). The funding agency was not involved in any study processes.
REFERENCES
- Pedersen BK, Saltin B. Exercise as medicine – evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand J Med Sci Sports 2015; 25: 1–72. DOI: 10.1111/sms.12581
- Kraus VB, Sprow K, Powell KE, Buchner D, Bloodgood B, Piercy K, et al. Effects of physical activity in knee and hip osteoarthritis: a systematic umbrella review. Med Sci Sports Exerc 2019; 51: 1324–1339. DOI: 10.1249/MSS.0000000000001944
- Bannuru RR, Osani MC, Vaysbrot EE, Arden NK, Bennell K, Bierma-Zeinstra SMA, et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthritis Cartilage / OARS, Osteoarthritis Research Society 2019; 27: 1578–1589. DOI: 10.1016/j.joca.2019.06.011
- Moseng T, Dagfinrud H, van Bodegom-Vos L, Dziedzic K, Hagen KB, Natvig B, et al. Low adherence to exercise may have influenced the proportion of OMERACT-OARSI responders in an integrated osteoarthritis care model: secondary analyses from a cluster-randomised stepped-wedge trial. BMC Musculoskelet Disord 2020; 21: 236. DOI: 10.1186/s12891-020-03235-z
- Dobson F, Bennell KL, French SD, Nicolson PJ, Klaasman RN, Holden MA, et al. Barriers and facilitators to exercise participation in people with hip and/or knee osteoarthritis: synthesis of the literature using behavior change theory. Am J Phys Med Rehabil 2016; 95: 372–389. DOI:10.1097/PHM.0000000000000448
- Hurley M, Dickson K, Hallett R, Grant R, Hauari H, Walsh N, et al. Exercise interventions and patient beliefs for people with hip, knee or hip and knee osteoarthritis: a mixed methods review. Cochrane Database Syst Rev 2018; 4: Cd010842. DOI: 10.1002/14651858.CD010842.pub2
- Bunting JW, Withers TM, Heneghan NR, Greaves CJ. Digital interventions for promoting exercise adherence in chronic musculoskeletal pain: a systematic review and meta-analysis. Physiotherapy 2021; 111: 23–30. DOI: 10.1016/j.physio.2020.08.001
- Joseph KL, Dagfinrud H, Hagen KB, Nordén KR, Fongen C, Wold OM, et al. The AktiWeb study: feasibility of a web-based exercise program delivered by a patient organisation to patients with hip and/or knee osteoarthritis. Pilot Feasibility Stud 2022; 8: 150. DOI: 10.1186/s40814-022-01110-3
- Borg G. Psychophysical scaling with applications in physical work and the perception of exertion. Scand J Work Environ Health 1990; 16: 55–58. DOI: 10.5271/sjweh.1815
- Nelligan RK, Hinman RS, Atkins L, Bennell KL. A short message service intervention to support adherence to home-based strengthening exercise for people with knee osteoarthritis: intervention design applying the behavior change wheel. JMIR Mhealth Uhealth 2019; 7: e14619. DOI: 10.2196/14619
- Riebe D, Ehrman JK, Liguori G, Magal M. ACSM’s guidelines for exercise testing and prescription. Tenth edn. Philadelphia: Wolters Kluwer, 2018.
- Duong V, Daniel MS, Ferreira ML, Fritsch CG, Hunter DJ, Wang X, et al. Measuring adherence to unsupervised, conservative treatment for knee osteoarthritis: a systematic review. Osteoarthr Cartil Open 2021; 3: 100171. DOI: 10.1016/j.ocarto.2021.100171
- Moseng T, Dagfinrud H, Østerås N. Implementing international osteoarthritis guidelines in primary care: uptake and fidelity among health professionals and patients. Osteoarthritis Cartilage / OARS, Osteoarthritis Research Society 2019; 27: 1138–1147. DOI: 10.1016/j.joca.2019.03.010
- Bennell K, Nelligan RK, Schwartz S, Kasza J, Kimp A, Crofts SJ, et al. Behavior change text messages for home exercise adherence in knee osteoarthritis: randomized trial. J Med Internet Res 2020; 22: e21749. DOI: 10.2196/21749
- Loe H, Nes BM, Wisløff U. Predicting VO2peak from submaximal- and peak exercise models: the HUNT 3 fitness study, Norway. PLoS One 2016; 11: e0144873. DOI: 10.1371/journal.pone.0144873